
TOP-RATED PHYSICAL THERAPY FOR TENNIS ELBOW RELIEF IN NEW JERSEY & PENNSYLVANIA
If you’re feeling a sharp, nagging ache on the outside of your elbow every time you grip a coffee mug, turn a doorknob, or shake someone’s hand — you’re not imagining it. That’s tennis elbow, and it’s one of the most common overuse injuries we treat at Trinity Rehab. Our team knows how to treat tennis elbow effectively. The good news: physical therapy is the most effective, research-backed path to lasting relief, and you can start right away in New Jersey or Pennsylvania without a doctor’s referral.
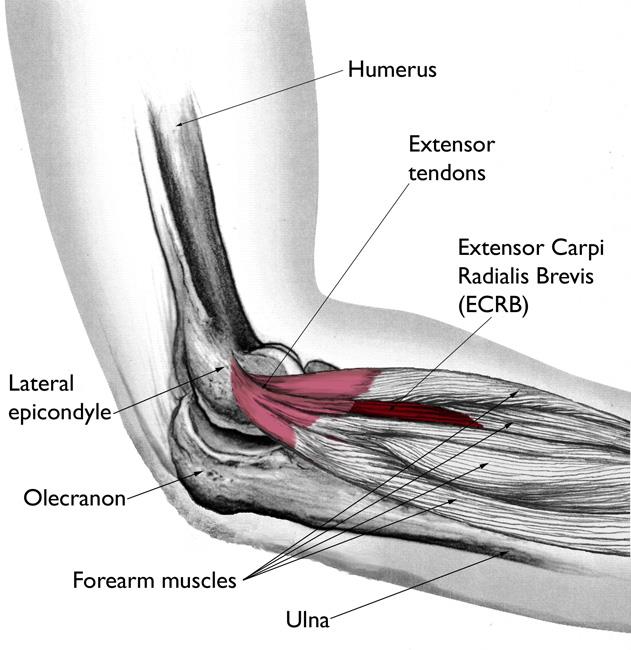
Tennis elbow (lateral epicondylitis) is a tendinopathy of the forearm extensor muscles — most often the extensor carpi radialis brevis (ECRB) tendon — where it attaches to the lateral epicondyle of the elbow. Despite the name, fewer than 5% of cases occur in tennis players. The overwhelming majority are caused by repetitive arm and wrist motions at work, at home, or in everyday activities.
This guide covers everything you need to know about tennis elbow management — what causes it, how physical therapy treats it, what exercises your therapist may prescribe, and how to choose the right provider. Our goal is to give you the clear, practical answers you need — so you can take the first step toward getting your arm back.

What Is Tennis Elbow (Lateral Epicondylitis)?
Tennis elbow — medically called lateral epicondylitis, or more precisely, lateral epicondylalgia (unilateral lateral epicondylalgia when it affects one arm) — is a painful condition affecting the tendons on the outer side of the elbow. It develops when the tendons connecting your forearm muscles to the bony bump on the outside of your elbow (the lateral epicondyle) become overloaded, irritated, and begin to degenerate.
Modern clinical research classifies tennis elbow as a lateral elbow tendinopathy rather than a true inflammatory condition. The tissue undergoes a process called angiofibroblastic degeneration — microscopic tears and structural changes within the tendon that reduce its load-bearing capacity. This is why anti-inflammatory approaches like ice and NSAIDs often provide only temporary relief: the problem isn’t primarily inflammation, it’s tendon degeneration that requires progressive loading through physical therapy to properly heal. Without appropriate rehabilitation, scar tissue can form around the damaged tendon fibers, limiting flexibility and increasing the likelihood of re-injury.
The primary tendon involved is the extensor carpi radialis brevis (ECRB), which controls wrist extension and stabilizes the wrist during gripping. Secondary involvement of the extensor digitorum and other forearm extensor muscles is common, as these muscles share the common extensor origin. When this tendon attachment is damaged, nearly every gripping and lifting movement becomes painful.
Who Gets Tennis Elbow? (It's Not Just Tennis Players)
Tennis elbow is one of the most misunderstood conditions in musculoskeletal medicine — because the name is almost entirely misleading. According to the American Physical Therapy Association’s choosept.com guide, fewer than 5% of tennis elbow cases actually occur in tennis players. The condition affects roughly 1–3% of adults overall, most commonly between the ages of 30 and 60.
The real risk factors are repetitive forearm and wrist motions and repetitive movement patterns performed over time. People who develop tennis elbow from repetitive movement include:
- Carpenters, plumbers, and painters — repetitive gripping, hammering, and twisting
- Office workers and computer users — sustained mouse use and keyboard work
- Cooks and butchers — repetitive chopping and gripping motions
- Healthcare workers — patient handling and instrument use
- Musicians — sustained forearm positioning while playing
- Mechanics — tool use requiring forearm rotation
- Gardeners — pruning, raking, and digging
- Warehouse and assembly workers — repetitive lifting that loads the forearm, often combined with knee, back, and shoulder strain
In other words, tennis elbow is a work-related musculoskeletal disorder and repetitive strain injury (RSI) that can develop in virtually any occupation or activity involving repeated forearm loading. If your job or hobby requires you to repeatedly grip, twist, or lift with your wrist and forearm, you are in the risk group — whether or not you’ve ever held a tennis racquet.
Tennis Elbow vs. Golfer's Elbow: What's the Difference?
Tennis elbow and golfer’s elbow are often confused because they both involve elbow tendon pain — but they affect opposite sides of the arm and require different treatment approaches.
Tennis elbow (lateral epicondylitis) affects the outer (lateral) side of the elbow. Pain is felt at the bony bump on the outside and radiates down the forearm. The extensor muscles — responsible for pulling the wrist up and back — are involved.
Golfer’s elbow (medial epicondylitis) affects the inner (medial) side of the elbow. Pain is felt at the bony bump on the inside and may radiate toward the wrist. The flexor muscles — responsible for pulling the wrist down and forward — are involved. Both conditions involve overloaded muscles and tendon attachments.
Both are overuse tendinopathies, both respond well to physical therapy, and both are commonly seen in people who have never played the sport they’re named after. A skilled physical therapist will assess which condition is present and build a treatment program tailored specifically to the affected tendon group.
Signs and Symptoms of Tennis Elbow
Common Symptoms You'll Notice
Tennis elbow has a recognizable pattern of symptoms that typically develop gradually rather than from a single acute injury. Most patients describe a slow buildup of discomfort that eventually becomes hard to ignore.
The most common symptoms include:
- Lateral elbow pain — aching or burning at the lateral elbow, specifically on the outer side, at or just below the bony bump
- Forearm pain — pain that radiates from the elbow down the back of the forearm
- Grip weakness — difficulty holding objects, opening jars, or shaking hands without discomfort
- Pain with wrist extension — discomfort when bending the wrist backward or lifting the hand
- Pain with pronation/supination — twisting the forearm (like turning a screwdriver) is painful
- Tenderness at the lateral epicondyle — direct pressure on the outer elbow is sore to the touch
- Morning pain or stiffness — symptoms often feel worse first thing in the morning or after periods of rest
- Pinch grip pain — picking up small items between the thumb and fingers is uncomfortable, and extending the fingers against resistance reproduces pain
The condition typically affects the dominant arm, but both arms can be involved, particularly in people with bilateral occupational exposure.
When Symptoms Need Professional Attention
Many people try to “push through” tennis elbow, hoping it will resolve on its own. While mild cases can improve with rest and activity modification, there are clear signals that professional physical therapy evaluation is warranted:
- Pain that persists beyond 4–6 weeks despite rest
- Symptoms that interfere with daily tasks like cooking, dressing, or computer work
- Weakness that makes gripping or lifting unreliable
- Pain that wakes you from sleep
- Symptoms that have improved and relapsed multiple times
- Any numbness, tingling, or radiating pain into the hand (this may suggest radial nerve or posterior interosseous nerve involvement requiring differentiation)
Without treatment, tennis elbow can become a chronic condition lasting 12 to 24 months — or longer. Early physical therapy dramatically shortens recovery time and reduces the risk of recurrence.
What Causes Tennis Elbow?
Repetitive Motion at Work
The root cause of tennis elbow is cumulative mechanical overload on the ECRB tendon and the common extensor origin. This occurs when the forearm extensor muscles are asked to perform the same movements repeatedly, often under load, without sufficient recovery time between bouts.
At work, the highest-risk activities include:
- Sustained computer mouse use (particularly with the arm unsupported)
- Repeated lifting with the palm facing down
- Vibrating tool use (jackhammers, drills, grinders)
- Sustained gripping in awkward forearm positions
- Overhead work requiring wrist extension against resistance
Ergonomic factors amplify risk significantly. A workstation where the arm is unsupported, the wrist is deviated, or the worker must reach across their body to operate equipment loads the ECRB in non-neutral positions — accelerating tendon degeneration over time.
Sports and Recreational Activities
While not the majority of cases, sports do contribute. In racquet sports, faulty technique is a major driver:
- Backhand technique errors — hitting with a “leading elbow” or poor shoulder rotation
- Grip size mismatch — grip that is too small or too large increases forearm tension
- Racquet string tension — overly tight strings transfer more vibration to the elbow
- Late ball contact — striking the ball behind the body increases wrist extension load
Beyond tennis, golfers (particularly with iron shots), fly fishermen, rock climbers, and CrossFit athletes are also commonly affected due to repeated or sustained forearm loading.
The Anatomy Behind the Pain
Understanding why tennis elbow is so stubborn requires a brief look at the anatomy involved.
The lateral epicondyle is the bony prominence on the outer side of your elbow. Multiple forearm extensor muscles — including the ECRB, extensor digitorum, extensor carpi radialis longus, and others — share a common tendon attachment at this point called the common extensor origin.
The ECRB is the primary culprit because of its position: it spans both the elbow and the wrist, is under constant tension during wrist extension and gripping, and is mechanically stressed each time the elbow is extended under load. Repeated microtrauma at the tendon-bone junction causes the process of angiofibroblastic degeneration — where the tendon’s normal collagen fibers are replaced by disorganized, weaker scar-like tissue. The tendon loses its tensile strength, becomes hypersensitive, and eventually becomes painful with loads it previously tolerated easily. Rebuilding tendon tolerance through graduated loading is the primary goal of physical therapy.
Critically, this degenerative process does not respond to rest alone. The tendon needs progressive, controlled loading — the cornerstone of physical therapy — to stimulate proper collagen remodeling and restore tensile strength.
How Physical Therapy Treats Tennis Elbow
Physical therapy is the first-line, evidence-based treatment for lateral epicondylitis. Research published through the American Physical Therapy Association (APTA) demonstrates that patients who receive early physical therapy for tennis elbow save an average of $10,739 compared to those managed with steroid injections over the course of their care — while also achieving better long-term outcomes. (choosept.com)
At Trinity Rehab, your tennis elbow treatment follows a structured, phase-based rehabilitation protocol tailored to your severity, goals, and activity demands.
Phase 1 — Acute Pain Management (Weeks 1–3)
The first phase focuses on reducing pain and protecting the tendon from further aggravating load while beginning the healing process.
Your physical therapist will:
- Perform a thorough evaluation including range of motion, strength testing, functional assessment, and pain behavior mapping
- Use manual therapy techniques including soft tissue mobilization, myofascial release, and Cyriax deep friction massage to reduce pain and improve tissue mobility around the common extensor origin
- Apply therapeutic modalities such as ultrasound, electrical stimulation (TENS/NMES), or dry needling to calm pain sensitivity, reduce inflammation in surrounding tissues, and promote healing at the tendon insertion
- Introduce EPAT (Extracorporeal Pulse Activation Technology) — a non-invasive shockwave therapy that uses acoustic pressure waves to stimulate blood flow and collagen production in the degenerating tendon. Trinity Rehab is one of the few outpatient PT practices in NJ and PA with EPAT on-site
- Provide activity modification guidance — identifying which specific tasks are loading the ECRB most aggressively and teaching you how to modify them without completely stopping all activity
- Apply kinesiology taping or prescribe a counterforce brace (forearm strap) when appropriate to reduce tendon stress during daily activities
- Begin very gentle range-of-motion and low-load exercises to maintain mobility without provoking symptoms

Phase 2 — Strengthening and Conditioning (Weeks 3–8)
Phase 2 is where the real tendon remodeling happens. Progressive resistance exercises — especially eccentric exercises — are the most well-supported intervention for lateral epicondylitis in the current evidence base.
This phase includes:
- Eccentric wrist extension exercises — the gold standard for tendon remodeling (see exercise descriptions below)
- Progressive forearm strengthening moving from low-load isometric contractions to full dynamic resistance
- Wrist and forearm stretching protocols to restore flexibility
- Continuation and progression of manual therapy as needed
- Grip strengthening exercises progressed in a pain-guided manner
- Ergonomic assessment and workstation modification recommendations if occupational factors are involved
- Education on load management and tennis elbow management principles — understanding how to slowly return to demanding activities as symptoms improve, without re-injuring the tendon
Range of motion (ROM) should approach full symmetry with the unaffected side during this phase, and pain with resistance testing (measuring grip strength using a dynamometer or manual test) should begin to improve measurably, tracked using outcome measures like the PRTEE (Patient-Rated Tennis Elbow Evaluation).


Phase 3 — Functional Rehabilitation and Return to Activity
The final phase bridges the gap between clinical strength and real-world demands. The goal is full, pain-free return to all activities — whether that’s swinging a tennis racquet, returning to carpentry, or simply working at a computer all day without discomfort.
This phase focuses on:
- Sport-specific or work-specific training — replicating the exact forearm loading patterns of your activity
- Advanced strengthening with full range of motion against progressive loads
- Neuromuscular re-education to restore proper movement patterns and healthy movement mechanics that minimize recurrent overload
- Prevention education — movement correction, learning when to avoid activities that aggravate the tendon, equipment adjustments, warm-up protocols, and movement-based strategies, and strength maintenance programs to prevent recurrence
- Independent home exercise program to maintain gains after formal PT concludes
Most patients complete formal physical therapy within 6–12 sessions over 4–8 weeks. Chronic cases may require a longer course. The key measure of progress is not pain intensity alone but restoration of pain-free grip strength and confidence returning to full activity.

Tennis Elbow Exercises Your Physical Therapist May Prescribe
These exercises are among the most well-supported interventions for lateral epicondylitis recovery. While they are appropriate for most patients at the correct stage of recovery, always follow your physical therapist’s specific guidance on timing, load (starting from one repetition at low resistance), and progression.
Important: Begin exercises at a pain level of 0–3 out of 10. Mild discomfort during exercise is acceptable; sharp, escalating pain is not. Stop and consult your therapist if symptoms worsen.
1. Eccentric Wrist Extension (The Gold Standard)
Eccentric exercises — in which the muscle contracts while lengthening — are especially effective for tendon remodeling in lateral epicondylitis.
How to perform:
- Sit with your forearm resting on your thigh or a table, palm facing down, wrist at the edge
- Hold a light weight such as a small dumbbell (0.5–2 lbs starting weight)
- Extend your arm outward with your forearm resting on your thigh or table edge, then use your opposite hand to lift your wrist into full extension (wrist bent back)
- Slowly lower the wrist back down over 3–5 seconds, controlled by the affected forearm alone
- Perform 3 sets of 15 repetitions, once daily
- Progress weight by 0.5 lbs when you can complete all reps with pain no greater than 3/10 — this gradual increase builds tendon tolerance over time
This exercise directly loads the ECRB through its full range in a controlled eccentric contraction, stimulating the collagen remodeling that heals the tendon.
2. Wrist Flexion and Extension Stretches
Restoring flexibility in the forearm extensor and flexor muscle groups reduces tension at the tendon attachment.
Extension stretch (for tennis elbow):
- Extend your affected arm straight in front of you, elbow straight
- Point your fingers toward the floor (wrist in flexion)
- Gently increase the stretch by pulling the back of your hand toward your body with the opposite hand
- Hold for 30 seconds, repeat 3 times
- Perform 2–3 times per day, especially before and after activity
Flexion stretch:
- Extend your arm with the palm facing down
- Gently pull the back of your hand upward (wrist into extension) with the opposite hand
- Hold for 30 seconds, repeat 3 times
3. Forearm Pronation and Supination
Restoring pain-free rotation of the forearm is essential for functional recovery — virtually every gripping activity requires some degree of forearm rotation.
How to perform:
- Sit with your elbow bent at 90° and tucked against your side
- Hold a light hammer or weighted object (the weight should be at one end so there is some resistance)
- Slowly rotate your palm face-up (supination) as far as comfortable, hold 2 seconds
- Slowly rotate your palm face-down (pronation), hold 2 seconds
- Perform 3 sets of 15 repetitions in each direction
- Progress to heavier resistance as symptoms allow
This exercise strengthens the pronator and supinator muscles, restoring balanced forearm mechanics and reducing repetitive strain on the ECRB.
4. Grip Strengthening
Grip weakness is both a symptom and a consequence of tennis elbow — rebuilding grip strength is essential for functional recovery.
How to perform:
- Use a soft therapy putty, stress ball, or foam ball
- Squeeze firmly (not maximally) and hold for 5 seconds
- Release completely and rest 5 seconds
- Perform 3 sets of 15 repetitions, once or twice daily
- Progress to a firmer putty or ball and add light weight exercises as symptoms allow
Start at a pain level well below 3/10. If gripping is too painful initially, isometric wrist extension (pressing the back of your hand against a fixed surface without moving) can be used as a starting-point alternative.
5. Towel Twist
This functional exercise integrates both forearm rotation and grip strength in a pattern that closely mirrors the demands of daily tasks like wringing a mop, twisting a jar lid, or throwing a ball.
How to perform:
- Hold a hand towel at both ends
- Twist it in both directions — first wringing it as if squeezing water out, then reversing
- Perform 3 sets of 10–15 repetitions in each direction
- Progress by increasing the number of sets, then by performing the twist more slowly for added time under tension
This exercise is typically introduced in Phase 2–3 once grip strengthening is well tolerated. It is an excellent bridge to returning to sport or occupational activities.
Tennis Elbow Treatment Options Compared
Physical Therapy (First-Line Treatment)
Physical therapy is universally recommended as the primary treatment for tennis elbow by the APTA and leading clinical guidelines. It addresses the root cause of the problem — tendon degeneration requiring progressive loading — rather than simply masking symptoms.
Benefits of PT for tennis elbow:
- Addresses the underlying tendinopathy through guided exercise and manual therapy
- Restores full strength and function
- Educates on activity modification to prevent recurrence
- No side effects
- Covered by most major insurance plans
- In NJ, accessible without a physician referral (Direct Access)
- Research shows patients save an average of $10,739 compared to injection-based care pathways (choosept.com)
Success rate: Studies report 80–90% of lateral epicondylitis cases resolve with conservative care including physical therapy.
Corticosteroid Injections — Why They're a Short-Term Fix
Corticosteroid injections are one of the most commonly prescribed treatments for tennis elbow, yet the evidence increasingly shows they provide only short-term relief and may worsen long-term outcomes.
What the research shows: Corticosteroid injections typically produce faster pain reduction at 6 weeks compared to physical therapy — but by 26 weeks and 52 weeks, patients who received injections have significantly higher recurrence rates and worse functional outcomes than those treated with PT. Multiple randomized controlled trials support this finding.
Why injections fail long-term: Corticosteroids reduce inflammation and pain temporarily, but they do not address the underlying tendon degeneration. While the inflammation reduction is real, the relief doesn’t last. Some evidence suggests repeated cortisone injections may further weaken the tendon matrix, increasing the risk of tendon rupture and chronic tendinopathy.
The appropriate role for corticosteroid injections is short-term symptom relief in severe acute pain — not as a standalone treatment or repeated therapy. If you’ve had one or more injections without lasting improvement, physical therapy is the appropriate next step.
PRP Therapy
Platelet-rich plasma (PRP) injections involve injecting a concentration of your own blood platelets into the affected tendon to stimulate healing. PRP for tennis elbow has shown promising results in several clinical trials, particularly for chronic cases that have failed conservative care.
PRP appears to produce better long-term outcomes than corticosteroid injections for chronic lateral elbow tendinopathy, though evidence is still evolving. PRP is typically considered when physical therapy alone has not resolved the condition after 3–6 months. It is most effective when combined with a structured physical therapy program — not as a standalone treatment.
Counterforce Bracing and Splinting
A counterforce brace (also called a forearm strap or tennis elbow strap) is a simple device worn around the upper forearm that disperses the mechanical load away from the ECRB tendon attachment. It does not cure tennis elbow, but it can reduce pain during aggravating activities, allowing patients to maintain some function during recovery.
Appropriate use: Wear the brace during activities that provoke symptoms (computer work, tool use, sport). Remove it during exercise and rest periods. A counterforce brace is an adjunct to physical therapy — not a substitute for it.
A wrist splint may occasionally be used at night to maintain a neutral wrist position and reduce morning symptoms in acute-phase cases.
Surgery — When It's Actually Necessary
An orthopedic surgeon may recommend surgical intervention for lateral epicondylitis — typically involving debridement of the degenerative ECRB tissue — is reserved for a small minority of patients who have failed 6–12 months of comprehensive conservative management including physical therapy, bracing, and injection therapy.
Surgery for tennis elbow has a reported success rate of approximately 80–90%, but it is associated with significant recovery time (3–6 months to return to full activity) and is not always necessary. In most cases, a well-executed physical therapy program will resolve the condition without surgery.
If you’ve tried to treat tennis elbow conservatively for more than 6 months without meaningful improvement, ask your provider about a referral to an orthopedic specialist for evaluation.
How Long Does Tennis Elbow Take to Heal with Physical Therapy?
Recovery time is one of the most common questions patients ask — and one of the most variable answers in musculoskeletal medicine. The honest answer depends on several factors, but evidence-based estimates provide a useful framework.
For early-stage lateral epicondylitis (symptoms present less than 3 months): Most patients experience significant improvement within 6–12 weeks of beginning physical therapy. With consistent adherence to the exercise program, activity modification, and hands-on therapy, many return to full function in this timeframe.
For chronic lateral epicondylitis (symptoms present more than 3 months): Recovery typically takes 3–6 months of structured physical therapy. The tendon remodeling process takes time — you are rebuilding the structural integrity of degenerated collagen fibers, which cannot be rushed. However, most patients in this category achieve full or near-full recovery with appropriate PT.
Without treatment: Untreated tennis elbow can persist for 12–24 months on average, and some cases become permanent without proper rehabilitation. Research consistently shows that early physical therapy shortens recovery duration, reduces total healthcare costs, and lowers the risk of recurrence.
Factors that affect recovery speed:
- Duration of symptoms before starting PT (earlier is always better)
- Severity of tendon degeneration on imaging
- Ability to modify aggravating activities during recovery
- Consistency with the home exercise program
- Co-existing conditions (cervical radiculopathy, shoulder pathology, knee or lower extremity issues affecting overall movement patterns, etc.)
- Age and general health
Up to 90% of patients with tennis elbow recover within 12 months with appropriate treatment. If you have been struggling longer than that, or if symptoms have repeatedly relapsed, a comprehensive physical therapy evaluation at Trinity Rehab can identify contributing factors and design a targeted recovery plan.
When Should You See a Physical Therapist?
You should consider scheduling a physical therapy evaluation if:
- Elbow pain has persisted for more than 4–6 weeks despite rest and over-the-counter anti-inflammatories
- Pain is affecting your ability to work, sleep, or perform daily tasks
- You’ve been told to “wait it out” or “rest more” but symptoms have not improved
- You’ve received a steroid injection but the relief has worn off
- Pain returns every time you try to return to your sport or activity
The sooner you start, the faster you’ll recover. Early physical therapy — before the condition becomes chronic — is associated with the best outcomes, fewest sessions required, and lowest total cost of care.
New Jersey Direct Access — No Referral Required
Under New Jersey’s Direct Access Act, you can schedule a physical therapy evaluation and begin treatment at Trinity Rehab without a doctor’s prescription or referral. You don’t need to wait for a physician appointment first.
What this means for you: You can call or book online today and be seen — often within the same week. Our physical therapists will perform a thorough evaluation, confirm the diagnosis, and begin treatment immediately. If imaging or specialist co-management is indicated, we will communicate with your physician.
Pennsylvania patients: Pennsylvania also permits direct access to physical therapy. Patients in our PA locations can schedule directly without a referral as well.
Most major insurance plans in NJ and PA are accepted. Our team will verify your benefits before your first visit.
Why Choose Trinity Rehab for Tennis Elbow Treatment?
One-on-One Personalized Care
At Trinity Rehab, you work with the same physical therapist throughout your entire course of care. This isn’t a high-volume clinic where you’re handed a sheet of exercises and left alone with a hot pack. Your therapist is with you during every session — evaluating your progress, adjusting your program, and providing hands-on manual therapy that makes a measurable difference in your recovery.
This consistency of care produces better outcomes. Your therapist knows your history, your job demands, your sport, and your goals. Your program evolves with you — from acute pain management through full return to activity.
Advanced Technology Others Don't Have
Trinity Rehab offers treatment modalities that most outpatient physical therapy clinics in New Jersey and Pennsylvania simply don’t have:
- EPAT (Extracorporeal Pulse Activation Technology) — non-invasive shockwave therapy that stimulates tissue healing in the ECRB tendon. Especially effective for chronic lateral elbow tendinopathy and lateral elbow pain that has not responded to conventional treatment
- Dry Needling — precise needling of the ECRB and surrounding forearm muscles to reduce pain sensitivity and promote healing at the tendon insertion
- AlterG Anti-Gravity Treadmill — while primarily used for lower extremity and post-surgical rehab, AlterG is part of our full-facility technology package representing Trinity Rehab’s commitment to advanced, evidence-based care
- Manual Therapy — hands-on joint mobilization, soft tissue mobilization, myofascial release, and instrument-assisted soft tissue mobilization (IASTM / Graston Technique) that accelerates recovery beyond exercise alone
Convenient Access and Insurance
| Feature | What We Offer | |—|—| | Scheduling | Early morning and evening appointments | | Insurance | In-network with most major NJ and PA insurance plans | | Direct Access | Start without a referral under NJ and PA law | | Locations | Multiple clinics across New Jersey and Pennsylvania | | Intake | Streamlined process with minimal paperwork |
We serve patients across New Jersey and Pennsylvania from multiple convenient locations. Whether you’re near our North Jersey, Central Jersey, or Pennsylvania clinics, expert tennis elbow care is close to home.
Trinity Rehab treats a full range of elbow, wrist, and hand conditions, as well as sports injuries and work-related injuries — making us the right choice whether your tennis elbow developed on the court or at your workstation.
Frequently Asked Questions
Related Conditions
How long does tennis elbow take to heal with physical therapy?
Can physical therapy fix tennis elbow?
What exercises help tennis elbow?
What causes tennis elbow in people who don’t play tennis?
When should I see a physical therapist for tennis elbow?
How long does tennis elbow last without treatment?
Is tennis elbow the same as golfer’s elbow?
What is the fastest way to cure tennis elbow?
Should I see a doctor or physical therapist for tennis elbow first?
How many physical therapy sessions are needed for tennis elbow?
Can tennis elbow heal on its own?
Does a tennis elbow brace (counterforce brace) actually help?
Find Tennis Elbow Treatment Near You
Trinity Rehab offers expert tennis elbow treatment at 27 convenient locations across New Jersey and Pennsylvania. Click your nearest clinic to learn more about local treatment options.
New Jersey
Pennsylvania
Tennis elbow is one of the most successfully treated conditions in physical therapy — but only when properly addressed. Waiting months or years for it to resolve on its own, relying on repeated steroid injections, or simply resting without a structured rehabilitation plan will keep you stuck in a cycle of pain and re-injury.
At Trinity Rehab, our physical therapists bring clinical expertise, advanced technology, and genuinely personalized care to every patient. You’ll work one-on-one with your therapist from your first evaluation through your return to full activity — with a program built around your specific demands, not a generic template.
And in New Jersey, you don’t need to wait for a doctor’s appointment first. Book directly under the Direct Access Act and start your recovery this week.
Sources:
OTHER CONDITIONS WE TREAT
Trinity Rehab treats a wide range of musculoskeletal conditions. Explore our other condition-specific resources: