ACL Recovery in Woodbridge, NJ: Complete Treatment, Rehab & Recovery Guide
When a high school athlete tears their ACL during Friday night football at Woodbridge High School, or a soccer player from Iselin’s competitive youth league goes down mid-season, the road to recovery feels impossibly long. But in Woodbridge—a township of over 103,000 people spread across nine distinct communities from Colonia to Port Reading—that recovery doesn’t have to be a lonely journey. At Trinity Rehab Woodbridge, located at 33 Woodbridge Center Drive in Crosspoint Town Square, we’ve helped hundreds of athletes and active residents return to the sports and activities they love.
An ACL (anterior cruciate ligament) injury is one of the most common and serious knee injuries, particularly among young athletes and active adults. But here’s the important truth: modern rehabilitation has transformed ACL recovery. Today, whether you choose surgery or conservative treatment, a structured physical therapy plan combined with culturally competent care adapted to Woodbridge’s incredibly diverse population can get you back in the game—often stronger and more resilient than before.
This comprehensive guide covers everything you need to know about ACL injuries, recovery timelines, rehabilitation phases, and why Woodbridge’s unique demographics and athletic landscape demand a specialized approach to treatment. We’ll explore the science behind ACL recovery, the practical steps you’ll take during rehabilitation, and why starting treatment immediately makes all the difference. Read on to understand your injury, explore your options, and take the first step toward getting back to what matters most to you.

What Is an ACL Injury? Understanding the Knee’s Most Critical Ligament
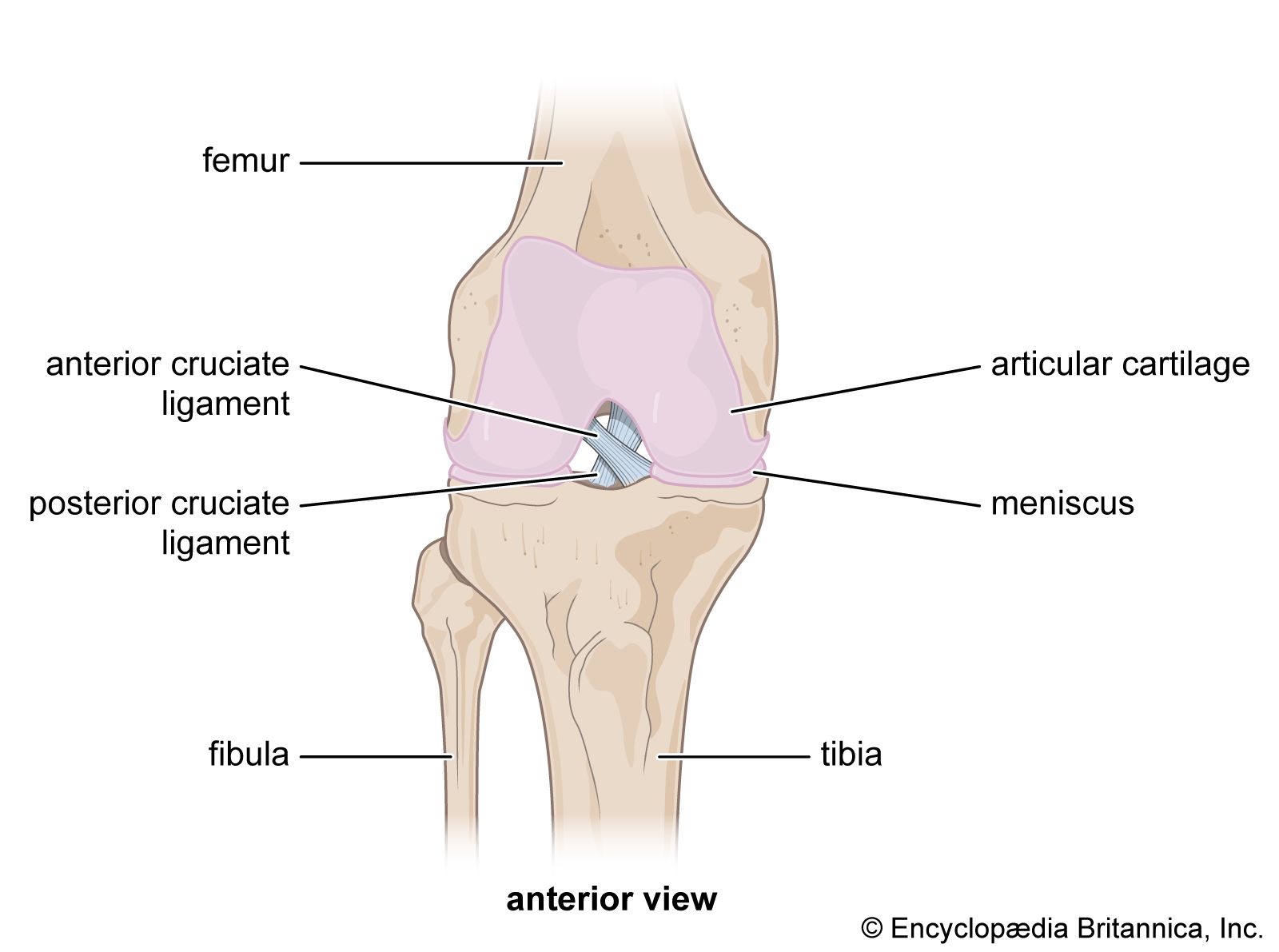
The anterior cruciate ligament (ACL) is one of four major ligaments that stabilize the knee joint. Located deep within the knee, the ACL runs diagonally from the femur (thighbone) to the tibia (shinbone), working alongside the posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL) to provide stability and control during movement.
Your knee is a hinge joint, primarily designed for forward and backward motion. But human movement demands much more: cutting, pivoting, twisting, and lateral movements. This is where the ACL becomes critical. When you hear a “pop” in your knee during a sudden direction change or a hard plant-and-cut movement—common in basketball, soccer, and football—there’s a good chance the ACL has partially or completely torn. That popping sensation is often the ACL fibers snapping.
An ACL injury is not like a simple muscle strain that heals on its own. It’s a structural injury to one of the knee’s load-bearing support systems. Unlike muscle, ligaments don’t have extensive blood supply, which means they heal slowly and never return to 100% of their original strength. This is why rehabilitation isn’t optional—it’s essential.
In Woodbridge, where the Greater Middlesex Conference brings together athletes from Woodbridge High School (the Barrons), JFK Memorial High School, and Colonia High School, we see ACL injuries across every sport: football, soccer, basketball, lacrosse, field hockey, volleyball, and baseball. These injuries don’t discriminate by age, gender, or athletic level. Young athletes competing at the high school level, weekend warriors at The Club at Woodbridge’s fitness facilities, and recreational sports players in Avenel, Fords, and Keasbey youth leagues all face the risk.
The ACL primarily prevents the tibia from sliding forward relative to the femur—a motion called anterior tibial translation. Without a functioning ACL, the knee becomes unstable and vulnerable to additional injuries, particularly to the meniscus (cartilage), which can lead to long-term degenerative changes. This is why prompt diagnosis and structured rehabilitation are so critical. The sooner you begin proper treatment, the better your long-term outcomes.
NJ’s Most Diverse Township and Culturally Competent ACL Care
Woodbridge Township stands out as New Jersey’s seventh most populous municipality and one of its most diverse communities. With a population of 103,639 and demographics that reflect the township’s multicultural character—44.6% White, 24.5% Asian, 12.2% African American, 9.3% multiracial, and 14.1% non-citizens—Woodbridge’s population brings distinctly different perspectives on injury, treatment, and recovery that directly impact how rehabilitation should be delivered.
At Trinity Rehab Woodbridge, we understand that a one-size-fits-all approach to ACL rehabilitation doesn’t work in a community as complex and varied as ours. Cultural competency in physical therapy isn’t about tokenism or box-checking; it’s about recognizing that injury recovery intersects with language, family expectations, spiritual beliefs, athletic traditions, and attitudes toward surgery and medical intervention. When these factors aren’t addressed, patients miss sessions, stop doing home exercises, or rush back to activity too early.
Language Barriers and Rehabilitation Instruction
For the 14.1% of Woodbridge residents who are non-citizens, and the many others for whom English is a second language, rehabilitation instructions can be confusing and frustrating. Imagine trying to understand the difference between an eccentric quad contraction (where the muscle lengthens while contracting, crucial for ACL recovery) and an isometric hold (where the muscle tightens without moving the joint) when terminology is being translated in real-time, or when printed materials use technical language you don’t fully grasp.
At Trinity Rehab, our team includes multilingual therapists and staff who can communicate rehabilitation protocols in Spanish, Mandarin, Gujarati, and other languages common to our community. Clear communication isn’t a luxury; it’s foundational to successful outcomes. We’ve found that patients who fully understand the purpose behind each exercise—not just the mechanics of how to do it—show significantly better adherence.
We also use visual demonstrations, written handouts in multiple languages, and video-based home exercise programs that don’t rely solely on verbal instruction. When a patient from Port Reading doesn’t fully understand why they need to avoid full knee extension for the first three weeks, or why pain-free range of motion matters more than pushing through discomfort, that gap in understanding can derail recovery. A patient might stop their home exercises thinking they’re “doing something wrong” when really they just didn’t understand the instruction. We eliminate that confusion.
Sports Traditions Across Communities
Woodbridge’s nine distinct communities—Woodbridge proper, Iselin, Colonia, Avenel, Port Reading, Sewaren, Fords, Hopelawn, and Keasbey—have different athletic traditions rooted in their demographic makeup. These aren’t trivial differences; they shape how patients experience their injury and what successful recovery looks like.
In Iselin and other neighborhoods with large South Asian populations, cricket and badminton are beloved recreational activities alongside traditional American sports. Cricket’s lateral movements, explosive changes of direction, and quick pivoting create specific ACL demands that differ significantly from football. A rehabilitation plan for a recreational cricket player needs to account for the sport’s unique biomechanical demands—the explosive lunges required for quick singles, the lateral positioning required for fielding, and the rapid acceleration and deceleration required for running between wickets. Standard ACL rehab might get you back to walking, but cricket-specific rehab gets you back to competitive play.
In communities with larger Latin American populations, soccer is the sport of choice and cultural identity. Soccer involves continuous lateral movement, frequent jumping, and rapid deceleration—ACL risk factors that our therapists must address directly. The competitive intensity and cultural significance of soccer in these neighborhoods means patients are highly motivated to return to play but may need realistic timelines about when that’s safe. We work with these athletes to establish phased return-to-sport protocols that honor their passion while protecting their knee.
In neighborhoods like Woodbridge proper and those surrounding Woodbridge High School, football, basketball, and lacrosse dominate. These contact sports and cutting sports place enormous ACL demands and sometimes involve cultural expectations about “tough it out” mentality that can actually hinder recovery if not addressed directly. We educate coaches and athletes about the difference between being tough and being smart; returning too early isn’t brave, it’s risky.
Varying Attitudes Toward Surgery Versus Conservative Treatment
Cultural background significantly influences whether a patient opts for ACL reconstruction surgery or pursues non-surgical rehabilitation. Some communities view surgery as the “gold standard” and feel uneasy pursuing conservative treatment, seeing it as somehow lesser. Others approach surgery cautiously, preferring to avoid it unless absolutely necessary, viewing it as an unnecessary risk. Neither perspective is right or wrong—but these attitudes must be addressed transparently during the initial consultation.
At Trinity Rehab Woodbridge, we present both pathways clearly, without bias or cultural assumptions. For some patients, surgery followed by structured rehabilitation is the right choice. For others—particularly those with lower functional demands or willingness to modify activities—high-quality conservative rehabilitation can be equally effective and appropriate. What matters is that the decision is made by the patient and their family with full information, not imposed by cultural assumptions or pressure from peers.
Why Culturally Aware PT Matters for Compliance and Outcomes
ACL rehabilitation requires compliance. You’ll need to attend 2-3 sessions per week for months. You’ll need to do home exercises daily. You’ll need to resist the urge to return to full activity before you’re ready. You’ll need to trust the process even when improvement feels slow. This level of commitment is easiest to maintain when the therapist understands your background, respects your timeline, and explains the “why” behind every phase.
Patients at Trinity Rehab Woodbridge who receive culturally competent care show better session attendance, higher adherence to home exercise programs, and faster progression through rehabilitation phases. When a therapist takes time to explain that returning to cricket too early might result in a second injury that could sideline you for two seasons—rather than just saying “don’t do jumping activities”—the message resonates differently. When we work with a patient’s extended family (common in many cultures) rather than just the individual patient, we create a support system that reinforces rehabilitation at home.
The Science Behind ACL Healing: Understanding Your Recovery Timeline
Before we discuss the practical phases of rehabilitation, it’s important to understand what’s happening in your knee at the biological level. ACL injuries trigger a specific healing response that unfolds over months. Understanding this timeline helps explain why rushing recovery is counterproductive.
The Healing Phases at the Cellular Level
- Immediate Phase (0-72 hours): When the ACL tears, blood vessels rupture and bleeding occurs in the joint. The body’s immediate response is inflammation—swelling that seems excessive but is actually protective. White blood cells rush to the injury, removing damaged tissue and bacteria. Inflammatory chemicals signal the body to begin repair processes. This is why swelling is normal and even beneficial in early phases; fighting it completely with excessive anti-inflammatory medication can slow healing.
- Inflammatory Phase (3 days to 3 weeks): The body produces fibrin, a protein that forms a scaffold for new tissue growth. Fibroblasts—cells that produce collagen—begin laying down new tissue. The ACL begins forming scar tissue, though this new tissue is initially weak and disorganized. The joint remains unstable; aggressive movement can disrupt the forming scar tissue and delay healing.
- Proliferative Phase (2 weeks to 3 months): New collagen is actively laid down. The ACL scar tissue strengthens, though it’s still immature and vulnerable. Proprioceptive nerve endings begin regenerating. This is why rehabilitation during this phase—with controlled loading and proprioceptive work—matters so much. The activities you do during this window literally shape how the new tissue organizes.
- Remodeling Phase (3 weeks to 12+ months): The new ACL tissue continues organizing and strengthening. Collagen becomes more densely packed and organized along the lines of force. The scar tissue never regains 100% of the original ligament’s strength, but it can become quite strong—strong enough to support athletic activity if rehabilitation is adequate.
This biological timeline explains the rehabilitation phases. You can’t speed it up with aggressive work; you’ll only disrupt healing. But you can optimize it with appropriate progressive loading and proprioceptive training.
Why Range of Motion Matters More Than Pain in Early Phases
Many patients expect that once pain decreases, they should progress their rehabilitation. Actually, range of motion is a better guide. Pain can be misleading. A movement might hurt without actually damaging tissue; conversely, some tissue damage might occur without much pain.
Early rehabilitation prioritizes regaining range of motion within pain-free limits because: (1) the ACL heals better when the knee is moving gently through its range; (2) stiffness that develops in early phases becomes much harder to address later; (3) proprioceptive nerve endings only regenerate if the joint is moving through its full range.
This is why early physical therapy is essential. A physician might tell you to “ice it and elevate it,” which is important, but it’s not sufficient. Gentle, progressive movement matters as much as rest.
Why ACL Recovery Matters: Getting Back to Your Life
An ACL injury isn’t just a sports injury, though that’s often how it’s framed. Yes, it affects your ability to compete. But it affects your confidence, your social connections, your mental health, your independence, and your overall quality of life in ways that extend far beyond sports.
For a 17-year-old Barron on the football team, an ACL injury represents uncertainty about college recruitment, team identity, and peer relationships. You’re sidelined while your teammates practice and compete. Friends who were your teammates have moved on. There’s genuine grief in that loss. For a 35-year-old from Colonia who plays recreational soccer on weekends, an ACL injury threatens one of their primary social outlets and stress-relief mechanisms. Soccer wasn’t just exercise; it was community and identity. For a 55-year-old who enjoys hiking and walking the trails near Woodbridge’s parks, an ACL injury creates fear of falling and instability that impacts daily life.
Proper rehabilitation addresses all of these concerns. It’s not just about returning to sport—it’s about returning to confidence, independence, and the life you want to live. When a 45-year-old can walk down stairs without pain or fear, when a high school athlete returns to the field with confidence in their knee, when a recreational player rejoins their team—that’s not just physical recovery, that’s life recovery.
Research consistently shows that comprehensive ACL rehabilitation improves not just knee function but also mental health, quality of life, and long-term outcomes. Patients who complete structured rehabilitation report higher satisfaction with outcomes and lower rates of re-injury compared to those who rush back or undertake inadequate rehabilitation.
Common Causes of ACL Injuries in Woodbridge
ACL injuries happen in specific ways. Understanding how your injury occurred helps us prevent re-injury and design rehabilitation that addresses your specific risk factors.
- Sports-related trauma: The most common cause of ACL injury is a sudden deceleration combined with a direction change. A basketball player plants their foot hard and cuts left. A soccer player jumps for a header and lands awkwardly on one leg. A football player makes a sharp cut and their knee stays planted while their body continues rotating. A lacrosse player decelerates suddenly to change direction. These are the classic ACL tear scenarios we see regularly at Trinity Rehab.
- Non-contact mechanisms: A player can tear their ACL without any contact—just from their own movement. Stopping suddenly, changing direction rapidly, or landing from a jump can be enough if forces exceed what the ligament can tolerate. In fact, approximately 70% of ACL injuries occur without any direct contact. This is important because it means improving movement quality can prevent injury.
- Contact injuries: Sometimes another player collides with the knee while it’s planted, forcing the knee into an unstable position. This is common in football (a defender hits the quarterback’s plant leg), basketball (an offensive player creates contact during a move), and soccer (collision while competing for the ball).
- Falls and accidents: Outside the sports context, ACL injuries happen from falls down stairs, slipping on ice, or motor vehicle accidents. Woodbridge winters mean icy sidewalks; we see our share of ACL injuries from falls on slick surfaces near Crosspoint Town Square and other shopping areas. Adults sometimes underestimate how a simple fall can damage the ACL.
- Overuse and biomechanical factors: Sometimes an ACL tear is the culmination of months of poor movement patterns, weak hip stabilizers, or inadequate rest. An athlete who hasn’t done proper strength training, who has significant muscle imbalances, or who increases training volume too quickly becomes vulnerable. The ACL can be thought of as a “last defense” against excessive stress; if your hips, core, and thighs aren’t strong enough, you’re asking your ACL to do more than it should.
Signs and Symptoms: Recognizing an ACL Injury
Not every ACL injury causes immediate, obvious pain or visible swelling. Some people report feeling a “pop” or hearing a “crack” at the moment of injury. Others describe immediate swelling, instability, or a sensation that the knee “gave out.” Some injuries are more subtle, with delayed symptoms developing over hours or days.
Immediate symptoms:
- Sharp pain in the knee at the moment of injury or within minutes
- A popping sensation or sound (described as a distinct “pop” that feels different from other joint sounds)
- Rapid swelling (usually within 2-3 hours as fluid accumulates in the joint)
- Instability or a feeling that the knee won’t support your weight
- Difficulty bearing weight on the injured leg
- Inability or severe difficulty continuing activity
- ACL treatment overview
Later symptoms:
- Persistent swelling that doesn’t resolve with basic ice and rest
- Knee pain with specific movements, particularly cutting or pivoting
- A feeling of instability or “the knee shifting” during lateral movements or when changing direction
- Limited range of motion, particularly difficulty straightening the knee fully
- Weakness in the leg, particularly with stairs, squatting, or walking on uneven surfaces
- Giving way: the knee suddenly feels unstable during normal activity
If you’ve experienced any of these symptoms—especially a pop followed by swelling—seek evaluation immediately. Early diagnosis and early rehabilitation, even before surgery if you choose that path, lead to better long-term outcomes. We recommend seeing an orthopedic surgeon or sports medicine physician within 48 hours of injury for proper evaluation.

Phase 1: Protection and Early Motion (Weeks 0-2 Post-Op)
The immediate post-operative phase focuses on protecting the surgical graft while preventing the knee from stiffening.
- Range of motion restoration: Gentle flexion and extension exercises to maintain knee motion without stressing the graft
- Quad activation: Isometric quadriceps contractions, straight leg raises, and neuromuscular electrical stimulation (NMES) to combat the rapid muscle shutdown that occurs after surgery
- Swelling management: Ice, compression, elevation, and manual lymphatic techniques
- Gait training: Progressing from crutches toward normalized walking patterns

How Physical Therapy Helps: The Complete ACL Recovery Roadmap
At Trinity Rehab Woodbridge, we approach ACL recovery through a structured, evidence-based framework grounded in current research and decades of clinical experience. Whether you’ve had ACL reconstruction surgery or are pursuing conservative management, your rehabilitation follows distinct phases. Each phase has specific goals, timelines, and criteria for progression. This isn’t arbitrary—the phases exist because the body heals in stages and the nervous system needs time to adapt.
Pre-Injury Prehab: The Best Injury Prevention
The best ACL injury is the one that never happens. For young athletes in Woodbridge’s three high schools and recreational leagues, ACL prehab—neuromuscular training before injury—significantly reduces ACL injury risk.
Prehab focuses on:
- Single-leg balance and proprioception: Building the neurological awareness that keeps knees stable during unexpected movements or when the ground is uneven. This includes eyes-open and eyes-closed balance, balance on firm and unstable surfaces, and balance during arm or upper-body movements.
- Hip and core strength: Strong hips are the foundation of knee stability. When your hip stabilizers are weak, your knee compensates by working harder. Over time, this creates knee pain and injury. Prehab emphasizes hip abductors, hip external rotators, and core muscles.
- Eccentric loading: Training muscles to control deceleration. Many ACL injuries happen during the deceleration phase of movement, not the acceleration phase. Athletes need to be strong during eccentric loading—the controlled lengthening of muscle under tension.
- Landing mechanics: Teaching athletes to land from jumps safely. Poor landing mechanics—knees caving inward, body weight forward over toes, inadequate hip control—predispose to ACL injury. Athletes who land with knees out, hips back, and balanced body weight rarely tear ACLs.
- Agility and cutting drills: Preparing muscles and nervous system for sport-specific demands. Progressive cutting drills at increasing speeds train the neuromuscular system to handle directional changes safely.
Research shows that 15-20 minutes of prehab training, done 3-4 times weekly, reduces ACL injury risk by up to 50%. This is especially important for athletes in the Greater Middlesex Conference, where competitive intensity is high. We offer prehab programs for high school athletes, recreational league players, and anyone interested in injury prevention.
Phase 1: Immediate Post-Injury or Post-Surgery (Weeks 0-2)
The first two weeks set the foundation. Whether you’ve just suffered the injury or just had surgery, the goals are identical: reduce swelling, restore normal walking, and begin regaining basic range of motion. This phase is about protection and gentle mobilization, not aggressive strengthening.
Typical protocols:
- Rest, ice, compression, elevation (RICE) to manage swelling—ice for 15-20 minutes, 3-4 times daily
- Crutches or a cane, as needed, to normalize walking pattern and protect the joint
- Gentle range-of-motion exercises: quad sets (tightening thigh muscles without moving knee), hamstring curls, ankle pumps
- Isometric quad strengthening: muscle activation without moving the joint—crucial for preserving muscle and maintaining nervous system connection
- Patellar mobility work: keeping the kneecap moving smoothly over the femur, important for long-term knee health
- Managing pain: working with your physician on appropriate pain management; some pain medication is appropriate in early phases
Milestones you’re aiming for:
- Reach 90 degrees of knee flexion (bending)—this is a critical threshold
- Walk without crutches in most situations
- Reduce swelling to manageable levels (knee girth not increasing throughout the day)
- Quad activation without pain—you should be able to tighten your thigh muscle without sharp pain
If you’ve had surgery, your surgeon may restrict certain movements during this phase. We work closely with your surgeon’s protocols to ensure safe progression. Communication between your therapist, surgeon, and you is essential.
Phase 2: Early Recovery (Weeks 2-6)
By week 2-3, you’ve moved beyond the injury’s acute phase. Now rehabilitation intensifies. Goals shift toward restoring full range of motion, building strength, and establishing proper movement patterns. This is when most people start to see tangible progress.
Typical protocols:
- Progressive range-of-motion work toward full extension (0 degrees) and full flexion (135+ degrees)
- Progressive strengthening: moving from isometric (no movement) to isotonic (with movement against resistance)
- Weight-bearing progression: gradually loading the leg more, advancing from toe-touch to partial weight to full weight
- Proprioceptive training: balance exercises on unstable surfaces, beginning to wake up the nervous system’s sense of position and movement
- Cardiovascular conditioning: stationary bike (with seat adjusted to allow pain-free motion), water walking, other low-impact options to maintain fitness without stressing the knee
- Swelling management: continued ice, elevation as needed, compression garment use
Exercises during Phase 2 typically include:
- Standing knee extensions with resistance bands (quadriceps strengthening)
- Hamstring curls with resistance (supine or standing)
- Standing hip abduction and adduction with resistance bands
- Step-ups or step-downs starting with 2-4 inch height
- Double-leg stance balance work progressing to single-leg (holding onto support)
- Stationary bike work with progressively increased resistance and duration
- Quadriceps isometric holds with progressive increases in duration
- Prone hip extension (glute strengthening)
Milestones you’re aiming for:
- Full knee extension (0 degrees) without pain—this is essential
- Knee flexion to at least 120-130 degrees, working toward 135+
- Single-leg stance for 30 seconds while holding onto support
- Quad strength at 4/5 on manual muscle testing (therapist assessment)
- Walking without swelling increase—if your knee swells after activity, you’ve done too much
- Confidence walking stairs with support

Phase 3: Progressive Strengthening (Weeks 6-12)
By week 6, most people can begin more dynamic activities. This is when rehabilitation transitions from pure rehabilitation to strength training that approaches normal activities. You’re building the strength foundation you’ll need for sport-specific work.
Typical protocols:
- Full-range strengthening exercises with progressive resistance
- Progressive resistance training using weights, bands, or body weight
- Balance and proprioceptive training on more challenging surfaces (balance board, foam pad, unstable surfaces)
- Introduction to dynamic activities (controlled movement patterns)
- Sport-specific movement patterns, modified (not yet at full speed)
- Cardiovascular conditioning progression—longer duration, higher intensity than Phase 2
Exercises during Phase 3 typically include:
- Squats starting shallow (quarter squats) and progressing to deeper depth as tolerated
- Lunges starting stationary and progressing to walking lunges
- Step-ups with increased height (6-8+ inches)
- Deadlifts with light weight, focusing on proper form
- Single-leg stance on unstable surfaces (balance pad, foam)
- Single-leg balance with upper-body movement (reaching arms, throwing movements)
- Lateral band walks (hip abductor strengthening in standing)
- Calf raises (single and double leg)
- Hamstring strengthening with various resistance methods
- Core strengthening: planks (front and side), side planks, dead bugs, bird dogs
- Stationary bike with progressive resistance and interval work
Milestones you’re aiming for:
- Squats to 90 degrees without pain or swelling
- Single-leg stance for 60+ seconds with minimal upper-body support
- Walking lunges with proper form across the gym
- Quad and hamstring strength at 4+/5 on manual muscle testing
- Single-leg balance with eyes closed for 30+ seconds
- Stairs no longer painful—you walk normally, not favoring the leg
Phase 4: Intermediate Strengthening & Power Development (Months 3-6)
Months 3-6 mark a transition into sport-specific preparation. Rehabilitation now includes plyometrics (jumping and explosive movements), agility work, and sport-specific drills that prepare your neuromuscular system for the demands you’ll face. This is when athletes start to feel like athletes again.
Typical protocols:
- Progressive plyometrics: jumping, bounding, directional changes at controlled speed
- Agility and speed training: cone drills, shuttle runs, figure-8 patterns
- Sport-specific movement patterns at moderate speed
- Continued strength training with higher intensity and progressive resistance
- Balance training with dynamic components—balance while moving, balance while reaching
- Cardiovascular conditioning at higher intensities—interval training, longer durations
Exercises during Phase 4 typically include:
- Double-leg hops and bounds in straight lines
- Single-leg hops for distance (measuring progress)
- Lateral bounds and cone drills (figure-8 patterns)
- Figure-8 running around cones at progressive speeds
- Cutting drills at 45 and 90 degrees at controlled speed
- Shuttle runs (sprinting, stopping, reversing direction)
- Jump-and-hold landings (jump and stick the landing with good form)
- Box jumps with progressive height
- Skater jumps (lateral jumping in lateral bound pattern)
- Continued strength training: weighted squats, deadlifts, lunges with progressive resistance
- Sport-specific drills: for basketball players, shooting drills with cutting; for soccer players, ball control drills with direction changes; for football players, pass-catching drills with footwork
Milestones you’re aiming for:
- Pain-free plyometric activities—no pain during or after jumping
- Able to perform cutting drills at moderate speed (60-75% of full speed)
- Quad and hamstring strength at 5/5 on manual muscle testing (full strength)
- Hamstring-to-quad ratio adequate for sport (typically 60-80%)
- Confidence in lateral movement—you trust your knee during side-to-side activities
- Single-leg hop test at 80%+ symmetry with uninvolved leg
Phase 5: Advanced Activity & Return to Sport (Months 6-9+)
The final phase is about matching or exceeding your pre-injury performance level and returning to sport safely. This phase includes sport-specific training at game intensity, return-to-sport testing, and psychological readiness assessment. It’s not just about physical capacity; it’s about confidence.
Typical protocols:
- Sport-specific training at game intensity and speed
- Return-to-sport testing: formal strength, power, agility, and proprioception assessment
- Psychological readiness assessment: confidence, fear of re-injury, motivation
- Sport-specific scenarios and competition simulation
- Maintenance strengthening and conditioning that continues beyond return
Return-to-sport considerations:
- Knee strength symmetry: involved leg at 90%+ of uninvolved leg
- Hamstring-to-quad ratio: 60-80% for safe ACL function
- Hop test symmetry: single-leg hop for distance 85%+ of uninvolved leg (objective test of power)
- Y-Balance Test: good stability in all directions
- Sport-specific skill proficiency at game speed and intensity
- Psychological readiness: confidence in knee, willingness to compete, minimal fear of re-injury
Timeline clarity:
- Non-surgical rehabilitation: 4-6 months to sport return
- Post-surgical rehabilitation: 6-9 months to sport return
- Some high-demand sports may require 9-12 months
Not all athletes return at the same rate. Some progress faster; others need more time. The timeline above is a guide, not a guarantee. Return is based on objective testing, not time alone. We use standardized tests—not feelings or assumptions—to determine when you’re ready.
Non-Surgical Management: An Option Worth Considering
Not everyone needs surgery. This is an important fact that sometimes gets lost in conversations about ACL injuries. If surgery is “the standard,” then choosing not to have it can feel like you’re compromising your recovery. That’s not accurate.
Research from the past decade shows that high-quality rehabilitation can be as effective as surgery for people with lower functional demands or willingness to modify activities. This doesn’t mean non-surgical management is easier—it’s actually just as demanding, requiring exceptional commitment to rehabilitation.
Non-surgical candidates typically include:
- Older athletes or non-athletes who don’t intend to return to cutting/pivoting sports
- People willing to modify activities or avoid certain sports
- Those with good baseline strength and proprioception
- Individuals with psychological readiness for conservative management
- Those motivated to commit to rehabilitation for 4-6+ months
Non-surgical rehabilitation typically takes 4-6 months, involves the same phases outlined above, but emphasizes proprioception, strength, and movement strategy to compensate for the absent ACL. Success requires honesty about your goals: you may never return to the same sport at the same level, but you can return to pain-free, functional activities.
For surgical candidates, the typical timeline is 6-9 months post-surgery before return to sport. Surgery is appropriate for high-demand athletes, those with additional injuries, or those with psychological preference for surgical reconstruction.
Mega-Township Athletics: 3 Schools, 9 Communities, 1 ACL Challenge
Woodbridge Township presents a unique athletic and geographic landscape unlike most other New Jersey municipalities. With 103,000+ residents spread across nine distinct communities—Woodbridge, Iselin, Colonia, Avenel, Port Reading, Sewaren, Fords, Hopelawn, and Keasbey—all funneling their athletes into three high schools (Woodbridge High School, JFK Memorial High School, and Colonia High School), the athletic infrastructure creates specific challenges and opportunities.
The Geographic Challenge
Imagine being a soccer player from Hopelawn who attends Woodbridge High School. Your home is eight miles from campus. You participate in conditioning and team practice on campus. You’re recovering from an ACL tear, and your physical therapy is at Trinity Rehab Woodbridge, located conveniently at Crosspoint Town Square—but that’s still a 15-minute drive from home. This geographic reality affects recovery in ways most cities don’t face.
Warm-up and cool-down logistics: Athletes commuting 20-30 minutes to practice or competition have less time for proper warm-up and cool-down. A 20-minute commute means you arrive with 5 minutes to spare instead of 15 minutes to properly warm up muscles and prepare your nervous system. Inadequate warm-up increases injury risk; inadequate cool-down impairs recovery and increases inflammation. We coach Woodbridge athletes on time-efficient warm-up protocols they can do in vehicles or on the drive and provide cool-down strategies that can be done at home or in vehicles after practice.
Recovery timing: A player from Port Reading finishing practice at Woodbridge High has a 30-minute commute home. By the time they’re home, icing and elevation—critical immediately post-workout—are delayed. Inflammation accumulation in the first 2-3 hours after activity is substantial. We discuss ice-pack strategies that work during commutes and emphasize same-day ice as part of daily routine.
Sleep and recovery: Early morning drives to school or practice, plus evening activity, mean some Woodbridge athletes have disrupted sleep schedules. Early morning practices or training sessions mean 6 AM alarms. Evening competitions or late practices mean arriving home at 9-10 PM. We help players adjust sleep schedules and emphasize sleep as a recovery tool as important as any exercise.
The Talent Pool and Competitive Intensity
With three competitive high schools in one township, the Greater Middlesex Conference is fiercely competitive. Athletes from Fords, Keasbey, Hopelawn, and other smaller communities integrate into larger Woodbridge High and JFK Memorial programs. This creates enormous talent pools but also intense competition and a culture where “playing through pain” is normalized.
High school athletes in Woodbridge are often more talented, more dedicated, and more competitive than average. This is good for athletic achievement but creates pressure to return too quickly. Coaches feel roster pressure. Players feel pressure from teammates and coaches. Parents want their child back in the game. This cultural environment—while understandable—can push athletes to return before they’re ready.
At Trinity Rehab Woodbridge, we address this head-on. We work directly with coaches and athletes to reframe ACL recovery not as weakness or lost time, but as intelligent investment. An athlete who returns prematurely risks a second ACL injury—a far more serious prospect. We help coaches understand that the player sitting out the next four weeks might otherwise miss the next four seasons. Re-injury rates are substantial for athletes who return before ready; re-injury means another surgery, another long rehabilitation, and potentially career-ending consequences.
We also work with parents, many of whom don’t understand ACL injury severity. We explain that ACL is not a “bump on the knee”—it’s a significant structural injury. An athlete returning at 80% strength to a sport demanding 100% performance is a recipe for disaster.
Supporting the Entire Community
Woodbridge isn’t just about high school athletics. The Club at Woodbridge provides fitness facilities used by adults throughout the township. Youth recreational leagues operate across all nine communities. Weekend warriors, older adults, and recreational athletes face ACL injuries too, though they may not have coaching staff pushing them to return early.
At Trinity Rehab Woodbridge, we serve everyone. A 45-year-old from Avenel recovering from an ACL tear during recreational basketball gets the same evidence-based, culturally competent care as a Barron varsity football player. The phases are the same; the sport-specific demands may differ. The psychological support is equally important. But the commitment to getting you back safely is identical.
For recreational athletes, return to sport might mean joining a recreational league, not competing at varsity level. That’s appropriate and successful. Success is defined by your goals, not by external standards.
Why Choose Trinity Rehab Woodbridge for ACL Recovery?
Located at 33 Woodbridge Center Drive in Crosspoint Town Square, Trinity Rehab Woodbridge isn’t just a physical therapy clinic. We’re a specialized ACL recovery center embedded in your community.
Our advantages:
- Specialized expertise: Our therapists hold specialized certifications in orthopedic rehabilitation and sports physical therapy. We’re not generalists treating ACL injuries alongside rotator cuff tears and back pain. ACL recovery is our specialty. We stay current on research and continuously refine our protocols.
- Culturally competent care: We understand Woodbridge’s demographic diversity. We have multilingual staff, use translated materials, and adapt communication styles to ensure every patient fully understands their rehabilitation. We understand that a South Asian cricket player’s injury demands differ from an African American basketball player’s demands, and we treat rehabilitation accordingly.
- Sport-specific expertise: Whether you’re a Barron, a recreational soccer player, or a cricket enthusiast, we have experience with your sport’s specific demands. Our therapists work with local schools and leagues. We understand the Greater Middlesex Conference’s competitive intensity.
- Evidence-based approach: Every exercise, every progression, every timeline is grounded in current research. We don’t follow outdated protocols. We use objective testing—strength measurements, hop tests, balance assessments—to determine readiness for progression, not guesswork or time-based progression.
- Comprehensive care: We coordinate with your physician and surgeon (if applicable). We communicate with your coaches. We provide support for the psychological aspects of recovery, not just the physical. We understand that returning from ACL injury involves confidence-building alongside strength-building.
- Convenient location: At Crosspoint Town Square, we’re accessible from all nine Woodbridge communities. Ample parking means you’re not circling for spaces. Our hours accommodate student-athletes, working adults, and retirees.
- Modern equipment and facilities: We have everything needed for comprehensive ACL rehabilitation—from basic range-of-motion work to advanced plyometrics to sport-specific training. Our facilities are equipped for every phase of rehabilitation.
Inside Our Woodbridge Clinic




Woodbridge ACL Rehab For Strength, Stability, And Return To Activity
ACL rehab in Woodbridge should connect the healing stage to real movement goals: walking normally, using stairs, rebuilding quad strength, returning to running, and feeling ready for sport or exercise again.
Your therapist may assess swelling, range of motion, quad activation, hip strength, balance, gait, and return-to-sport readiness. The plan should match your surgical or non-surgical timeline and avoid skipping phases.
Related options include knee pain physical therapy, meniscus tear rehab, and the Woodbridge physical therapy clinic page.
Frequently Asked Questions About ACL Injury and Recovery
Woodbridge ACL Rehab For Strength, Stability, And Return To Activity
ACL rehab in Woodbridge should connect the healing stage to real movement goals: walking normally, using stairs, rebuilding quad strength, returning to running, and feeling ready for sport or exercise again.
Your therapist may assess swelling, range of motion, quad activation, hip strength, balance, gait, and return-to-sport readiness. The plan should match your surgical or non-surgical timeline and avoid skipping phases.
Related options include knee pain physical therapy, meniscus tear rehab, and the Woodbridge physical therapy clinic page.
Do I definitely need surgery if I tear my ACL?
How long until I can return to sports?
What’s the difference between ACL and MCL injuries?
Can I do physical therapy if I don’t have surgery?
What should I do immediately after tearing my ACL?
Can I re-tear my ACL after recovery?
How much does ACL rehabilitation cost?
What if I’m not an athlete—will I still need intensive rehabilitation?
Can I do my home exercises instead of coming for therapy?
How do I know when I’m ready to return to sports?
Next Steps: Starting Your ACL Recovery Today
If you’re dealing with an ACL injury—whether diagnosed yesterday or nagging you for months—the time to act is now. Recovery is possible. Athletes return to sport. Non-athletes return to hiking, dancing, and playing with grandchildren. But recovery requires commitment, expertise, and the right support.
Here’s what we recommend:
Trinity Rehab Brick is ready to guide you through every phase of ACL recovery.
- Get a diagnosis if you haven’t already. An MRI confirms ACL injury and identifies any additional damage. See your primary care physician or an orthopedist within 48 hours of injury.
- Schedule a consultation at Trinity Rehab Woodbridge. Call us or visit our Crosspoint Town Square location at 33 Woodbridge Center Drive. We’ll discuss your goals, your sport, your lifestyle, and what recovery looks like for you specifically. We’ll answer questions and develop a plan.
- Commit to rehabilitation. Whether surgery or conservative treatment, recovery requires effort. Plan for 2-3 sessions weekly for several months. Plan for home exercises most days. This is your investment in returning to the activities you love.
- Trust the process. Rehabilitation has a proven timeline for a reason. Pushing too hard too fast risks re-injury. Following the plan, doing the work, and progressively challenging yourself—this approach works.
You live in Woodbridge, a diverse, athletic community with world-class fitness facilities and incredible talent. Whether you’re a Barron or a recreational player, a high school student or a 55-year-old weekend warrior, you deserve professional ACL care from people who understand your sport, your community, and your goals.
Trinity Rehab Woodbridge is here to get you back. Let’s start today.