ACL Recovery in Wayne, NJ: Complete Treatment, Rehab & Recovery Guide
If you’re an athlete in Wayne, New Jersey—whether you play varsity soccer at Wayne Hills, compete for a roster spot at Wayne Valley, spend your winters training at Ice Vault, or participate in one of Wayne PAL’s nationally recognized youth sports programs—an ACL injury can feel like your athletic career has come to a sudden halt. The anterior cruciate ligament (ACL) is one of the most critical structures in your knee, and when it tears, the impact on performance, confidence, and long-term joint health becomes immediately apparent. For young athletes in our community, where rivalry between high schools runs deep and year-round training starts as early as age five, ACL injuries represent a significant challenge. The good news? With the right physical therapy, structured rehabilitation, and professional guidance from Trinity Rehab’s Wayne location on Hamburg Turnpike, most athletes return to sport stronger and more resilient than before.
This comprehensive guide walks you through everything you need to know about ACL injuries, recovery, and returning to the sport you love—with specific insights tailored to Wayne’s unique athletic culture, from the intense two-school rivalry to the specialized demands of ice sports at our local Ice Vault arena..

What Is an ACL Injury?
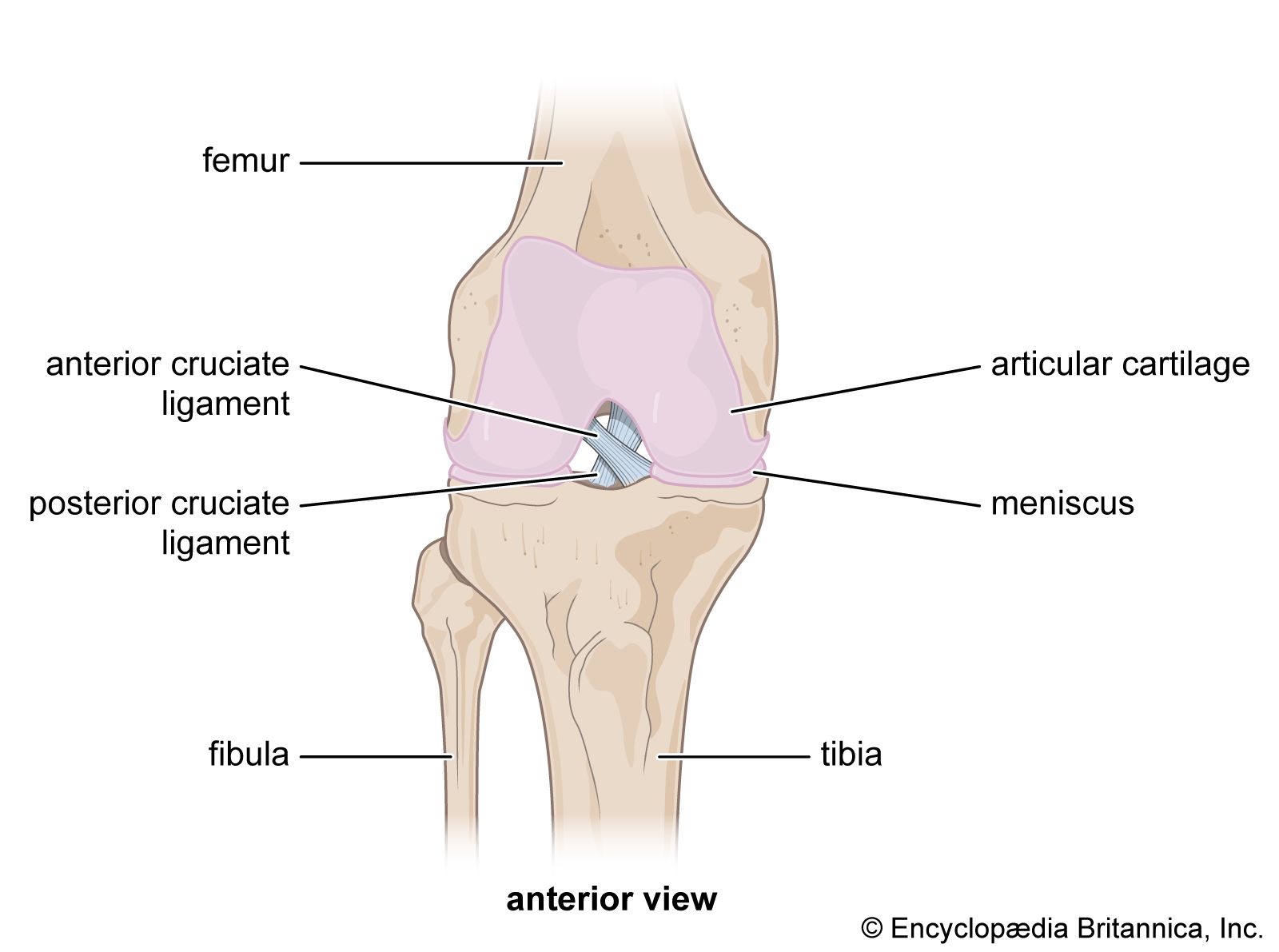
The anterior cruciate ligament is one of four major ligaments that stabilize your knee joint. It runs diagonally from your femur (thighbone) to your tibia (shinbone), providing crucial rotational stability and preventing your shin from sliding forward excessively. When you twist your knee with your foot planted, change direction rapidly at high speed, or experience a direct blow to the side of your knee, the ACL can tear—partially or completely.
ACL injuries are common among athletes because they often occur during movements that define competitive sports: a sudden pivot on the soccer field, a quick lateral cut while running for a rebound, an aggressive stop on ice skates, or a hard plant-and-turn in basketball. In Wayne, where our youth athletes are exposed to year-round training across multiple sports—baseball at the community diamonds, soccer during spring and fall, hockey during winter months, and recreational sports through Wayne PAL year-round—the cumulative stress on the ACL increases significantly.
The injury itself may occur with a “pop” sensation, immediate pain, and rapid swelling. However, some athletes experience a more subtle onset, noticing instability or a “giving way” sensation before they seek evaluation. This is why understanding the signs and symptoms of an ACL injury is critical for early diagnosis and appropriate care.
The Two-School Rivalry and ACL Pressure: A Wayne-Specific Challenge
Wayne presents a unique athletic landscape unlike most New Jersey towns. Unlike communities with a single high school feeding one athletic program, Wayne’s athletes must navigate a phenomenon that creates distinctive pressure: the rivalry between Wayne Hills High School and Wayne Valley High School. This intra-town competition has deep roots in our community, creating not just athletic rivalry but also a competitive environment that shapes how young athletes train, specialize, and push their bodies year-round.
The impact of this two-school dynamic on ACL injury rates begins far earlier than high school. The Wayne PAL (Police Athletic League) organization—known nationally for excellence in youth sports—serves as the feeder system for both high schools. Athletes as young as five or six years old begin participating in organized, competitive sports through Wayne PAL’s baseball, soccer, football, basketball, cheerleading, and lacrosse programs. This early start to competitive athletics, while providing tremendous benefits, also creates training intensities that were historically reserved for older athletes.
The dual-school dynamic compounds this pressure in several ways. First, roster spots at both Wayne Hills and Wayne Valley are highly competitive. An athlete who might have been a certain starter or roster position at a town with one high school must compete against roughly twice as many equally talented peers. This translates directly into pressure to specialize early, train year-round, and push harder—earlier. Parents and coaches recognize that the competition for college recruitment attention is fiercer when scouts evaluate athletes from both Wayne high schools simultaneously.
Second, the “all-county” recognition structure in New Jersey basketball, soccer, football, and lacrosse becomes even more competitive when two schools from the same town are selecting players. Rather than one Wayne representative per position on county all-teams, both schools are vying for those same recognition slots. This drives overtraining—athletes feel compelled to perform in club sports, AAU organizations, and year-round competitive leagues to differentiate themselves.
Third, the developmental pressure filters down to youth levels. A seven-year-old playing in Wayne PAL knows that if they don’t stand out now, they’ll be competing against the other school’s youth athletes in a few years. This knowledge—explicit or implicit—drives both coaches and parents to invest in specialized training, private lessons, and increasingly intense practice regimens.
The consequence? Young athletes in Wayne experience ACL injury patterns that show earlier onset, higher rates of overuse injury preceding ACL tears, and increased incidents of return-to-sport ACL injuries compared to single-school communities. We’ve observed athletes at Trinity Rehab Wayne who suffered ACL tears at 14 or 15 because they were training like 17-year-olds—competing in fall soccer, winter basketball, spring baseball, and summer AAU tournaments simultaneously, with minimal off-season recovery.
Furthermore, the rivalry creates a psychological burden after ACL injury. An athlete from Wayne Hills who tears their ACL might face not only their own high school’s expectations for return, but also an awareness that their peers at Wayne Valley are advancing athletically during their recovery. This pressure to return “too soon” is significant. At Trinity Rehab Wayne, part of our counseling and education addresses this psychological dimension—helping athletes and families understand that returning to sport prematurely after ACL injury increases the risk of re-injury by 40-80%, depending on the study. A six-month recovery timeline, though it feels long when your cross-town rivals are playing, provides the structural and functional foundation necessary for safe, sustained return to sport.
We work with families to reframe the recovery narrative: an athlete who rehabilitates thoroughly and returns at 100% capacity has a competitive advantage over peers who returned too soon and are still managing instability or compensatory movement patterns. In a two-school rivalry where every advantage matters, this investment in proper rehabilitation pays dividends.
The Two-School Rivalry and ACL Pressure: A Wayne-Specific Challenge
Wayne presents a unique athletic landscape unlike most New Jersey towns. Unlike communities with a single high school feeding one athletic program, Wayne’s athletes must navigate a phenomenon that creates distinctive pressure: the rivalry between Wayne Hills High School and Wayne Valley High School. This intra-town competition has deep roots in our community, creating not just athletic rivalry but also a competitive environment that shapes how young athletes train, specialize, and push their bodies year-round.
The impact of this two-school dynamic on ACL injury rates begins far earlier than high school. The Wayne PAL (Police Athletic League) organization—known nationally for excellence in youth sports—serves as the feeder system for both high schools. Athletes as young as five or six years old begin participating in organized, competitive sports through Wayne PAL’s baseball, soccer, football, basketball, cheerleading, and lacrosse programs. This early start to competitive athletics, while providing tremendous benefits, also creates training intensities that were historically reserved for older athletes.
The dual-school dynamic compounds this pressure in several ways. First, roster spots at both Wayne Hills and Wayne Valley are highly competitive. An athlete who might have been a certain starter or roster position at a town with one high school must compete against roughly twice as many equally talented peers. This translates directly into pressure to specialize early, train year-round, and push harder—earlier. Parents and coaches recognize that the competition for college recruitment attention is fiercer when scouts evaluate athletes from both Wayne high schools simultaneously.
Second, the “all-county” recognition structure in New Jersey basketball, soccer, football, and lacrosse becomes even more competitive when two schools from the same town are selecting players. Rather than one Wayne representative per position on county all-teams, both schools are vying for those same recognition slots. This drives overtraining—athletes feel compelled to perform in club sports, AAU organizations, and year-round competitive leagues to differentiate themselves.
Third, the developmental pressure filters down to youth levels. A seven-year-old playing in Wayne PAL knows that if they don’t stand out now, they’ll be competing against the other school’s youth athletes in a few years. This knowledge—explicit or implicit—drives both coaches and parents to invest in specialized training, private lessons, and increasingly intense practice regimens.
The consequence? Young athletes in Wayne experience ACL injury patterns that show earlier onset, higher rates of overuse injury preceding ACL tears, and increased incidents of return-to-sport ACL injuries compared to single-school communities. We’ve observed athletes at Trinity Rehab Wayne who suffered ACL tears at 14 or 15 because they were training like 17-year-olds—competing in fall soccer, winter basketball, spring baseball, and summer AAU tournaments simultaneously, with minimal off-season recovery.
Furthermore, the rivalry creates a psychological burden after ACL injury. An athlete from Wayne Hills who tears their ACL might face not only their own high school’s expectations for return, but also an awareness that their peers at Wayne Valley are advancing athletically during their recovery. This pressure to return “too soon” is significant. At Trinity Rehab Wayne, part of our counseling and education addresses this psychological dimension—helping athletes and families understand that returning to sport prematurely after ACL injury increases the risk of re-injury by 40-80%, depending on the study. A six-month recovery timeline, though it feels long when your cross-town rivals are playing, provides the structural and functional foundation necessary for safe, sustained return to sport.
We work with families to reframe the recovery narrative: an athlete who rehabilitates thoroughly and returns at 100% capacity has a competitive advantage over peers who returned too soon and are still managing instability or compensatory movement patterns. In a two-school rivalry where every advantage matters, this investment in proper rehabilitation pays dividends..
Why Recovery Matters: Long-Term Health Beyond This Season
Many young athletes view an ACL injury through a single-season lens: “Will I play this year?” While returning to sport is important, the broader question—“Will my knee remain healthy for the next 20, 30, 40 years of my life?”—deserves equal attention.
Untreated or inadequately rehabilitated ACL injuries set athletes on a trajectory toward early-onset knee osteoarthritis (OA), typically beginning in the 30s or 40s. Research shows that ACL-deficient knees develop OA at nearly twice the rate of uninjured knees. Moreover, an athlete who tears their ACL and returns to sport without proper rehabilitation faces a 15-30% risk of tearing the opposite ACL within the first year—a phenomenon known as the “contralateral ACL rupture.”
But with appropriate physical therapy rehabilitation, athletes can not only return to their sport of choice but actually improve their overall athletic performance. Proper ACL rehab strengthens stabilizing muscles (quadriceps, hamstrings, glutes, hip stabilizers), improves proprioception and body awareness, and teaches movement patterns that reduce injury risk across all sports. Athletes we’ve treated at Trinity Rehab Wayne often report feeling more confident, stable, and explosive after successful rehabilitation than they did pre-injury.
The recovery process also provides an opportunity to address underlying movement deficits that may have contributed to the original injury. Many athletes in Wayne—particularly those specializing in a single sport—develop muscular imbalances or movement patterns that increase ACL injury risk. A soccer player might have weak hip abductors. A hockey player might compensate with excessive knee valgus (inward collapse). A basketball player might lack ankle mobility, shifting stress to the knee. Rehabilitation addresses these root causes, not just the ACL tear itself.
Common Causes of ACL Injuries in Wayne’s Athletic Community
ACL injuries occur through several primary mechanisms, and understanding which apply to your sport is valuable for prevention and recovery.
Non-Contact Pivot and Cut Injuries remain the most common cause (70% of ACL tears). These occur during sudden deceleration, rapid direction changes, or pivoting movements with the foot planted and the body rotating. For Wayne athletes, this includes: a soccer player planting to change direction while dribbling, a basketball player cutting hard on offense or defense, a field hockey player executing a stick turn, a lacrosse player dodging a defender. These injuries often occur without any collision—purely from the internal stress of the movement itself.
Direct Contact Injuries account for the remaining 30% of ACL tears. A defender’s tackle that drives into the side of the knee, a collision during a fast break, or even a fall during outdoor winter training on icy pavement can produce direct force that ruptures the ACL.
Ice Sports-Specific Causes deserve particular mention given Wayne’s Ice Vault arena and our community’s figure skating, hockey, and ice sports culture. ACL injuries in ice sports occur through: the sudden stopping force of ice hockey (a player stopping quickly to pivot), rotational movements in figure skating (particularly during jumps when landing mechanics fail), hip checks in hockey that drive the athlete’s knee into an unstable position, and falls where the blade catches the ice and the body continues rotating.
Overtraining and Fatigue create a significant risk factor in Wayne’s youth athletic culture. When athletes train 20+ hours per week across multiple sports and competitive organizations, muscular fatigue reduces the stabilizing force around the knee. Fatigued muscles recover more slowly from movements, leaving the ACL to absorb forces it normally wouldn’t. The Wayne PAL system, while excellent, places young athletes in competitive environments where coaches and parents sometimes push for increased intensity without adequate recovery. Overtraining is a silent contributor to ACL injuries.
Inadequate Prehab and Movement Screening also contribute. Athletes who lack sufficient hip and ankle mobility, who have weak glute muscles, or who have never been screened for movement deficits face higher ACL injury risk. Unlike some communities with robust athletic training programs, not all Wayne youth athletes have access to pre-participation movement screening or injury prevention training.
Signs and Symptoms: Recognizing an ACL Injury
Acute Presentation (immediate after injury):
- A sudden “pop” or tearing sensation in the knee
- Immediate, severe pain
- Rapid swelling within 2-4 hours (often described as the knee “blowing up”)
- Immediate loss of stability or sensation that the knee is “unstable” or “giving out”
- Inability to continue activity or bearing weight
- learn more about ACL treatment
Chronic or Gradual Presentation:
- Recurrent episodes of the knee “giving way” or instability during sports
- Pain with certain movements, particularly cutting or pivoting
- Swelling that develops after activity
- Weakness or the sensation that the leg “isn’t responding” during lateral movements
- Compensatory pain in the hip or opposite knee (from altering movement patterns)
In Youth Athletes: Young athletes sometimes underreport symptoms, particularly if they’re motivated to return quickly to sport. They might describe it as “my knee feels weird” or “it doesn’t feel stable during cuts” rather than reporting pain. Parents and coaches should take seriously any report of the knee feeling unstable or “wobbly,” even if the athlete minimizes other symptoms.
If you or your athlete experiences any of these signs, the first step is evaluation by a physician or physical therapist who can perform specific tests (Lachman test, anterior drawer test, pivot shift test) to assess ACL integrity.
How Physical Therapy Helps: Prehab, Five Phases of Rehabilitation, and Return-to-Sport
At Trinity Rehab Wayne, we’ve developed a comprehensive rehabilitation framework that guides athletes from injury through successful return to sport. This framework emphasizes that rehabilitation isn’t just about regaining range of motion or strength—it’s about restoring confidence, movement quality, and the specific physical demands of your sport.
Phase 1: Immediate Post-Injury (Weeks 0-2)
The first two weeks after ACL injury focus on managing swelling, protecting the knee, and restoring basic range of motion.
Goals:
- Reduce swelling and pain through RICE protocol (rest, ice, compression, elevation)
- Restore normal walking pattern
- Begin gentle range of motion exercises
- Activate quadriceps and hip muscles to prevent rapid muscle atrophy
Treatment Approaches:
- Manual therapy to mobilize the knee and restore gliding movements
- Cryotherapy (ice) and compression to manage swelling
- Quad sets and straight leg raises to activate thigh muscles
- Stationary cycling (if pain-free) at very low resistance
- Hip and ankle mobility work to prevent compensatory restrictions
- Home Program: Athletes perform ice application 3-4 times daily for 15-20 minutes, elevation when resting, and basic exercises for 10-15 minutes daily. We emphasize that this phase is about protection and gentle restoration, not pushing through pain.

Phase 2: Early Rehabilitation (Weeks 2-6)
As swelling decreases and weight-bearing tolerance improves, Phase 2 introduces more dynamic strengthening.
Goals:
- Restore full range of motion (0-130 degrees of knee flexion)
- Build strength in quadriceps, hamstrings, and hip musculature
- Improve walking mechanics and basic stability
- Progress to full weight-bearing without crutches
Treatment Approaches:
- Progressive strengthening: standing quad sets, hamstring curls, glute bridges, step-ups (low height)
- Balance training: double-leg stance progression to single-leg stance
- Stationary cycling with progressive resistance
- Swimming or pool walking (if appropriate for surgical or non-surgical timeline)
- Introduction of gentle movement patterns: mini-squats, side-stepping
Why This Phase Matters: The quadriceps muscle begins atrophying immediately after ACL injury. By Week 2, strength loss is already measurable. This phase reverses that trend, but it requires consistent effort. Young athletes often want to progress faster—especially in a competitive environment like Wayne where missing time feels costly. We emphasize that rushing this phase increases injury risk during later phases.

Phase 3: Functional Strengthening (Weeks 6-12)
Phase 3 introduces more sport-specific movements and greater demands on knee stability.
Goals:
- Achieve strength levels at 90% or greater compared to the uninjured leg
- Develop single-leg stability for dynamic movements
- Introduce directional changes and controlled pivoting
- Progress proprioceptive training (body awareness and balance)
Treatment Approaches:
- Single-leg strengthening: single-leg squats, single-leg deadlifts, single-leg calf raises
- Forward, lateral, and backward lunges with progressive load
- Resisted hip movements: clamshells, hip abduction, hip adduction
- Balance progression: single-leg stance on unstable surfaces, balance board training
- Introduction of light plyometric training: double-leg hops, small box steps
- Sport-specific movement patterns: lateral shuffles, forward/backward sprints (controlled)
Assessment: At the end of Phase 3, we conduct strength testing to ensure the involved leg has reached 90% strength compared to the uninjured side. This is not negotiable for progression—if strength is inadequate, the athlete remains in Phase 3 until improvement occurs.
Phase 4: Advanced Strengthening and Sport-Specific Training (Months 3-6)
Phase 4 bridges the gap between rehabilitation and sport. This is where young athletes in Wayne—eager to return to the field or ice—often feel renewed motivation.
Goals:
- Achieve strength levels at 95%+ compared to the uninjured leg
- Master multi-directional movements and rapid deceleration
- Develop confidence in the knee during sport-specific demands
- Return to sport-specific drills at controlled intensity
Treatment Approaches:
- Advanced plyometrics: bounding, single-leg hops, depth jumps, lateral bounding
- Sport-specific drills: for soccer players, directional changes with ball; for basketball players, defensive shuffles and cutting drills; for hockey players, skating starts and stops (if cleared); for figure skaters, controlled jumps and spins
- Agility ladder work, cone drills, and shuttle runs
- Eccentric strengthening (emphasized in this phase): downhill walking, slow-eccentric squats, step-downs
- Return to sport-specific training: initial team practice participation at modified intensity (50-75%)
The Psychological Component: This phase often brings psychological challenges. Athletes feel ready to “get back” but must respect load progression. We work with both athletes and coaches to develop return-to-sport plans that increase intensity gradually. A soccer player, for example, might begin with possession drills, progress to small-sided games, then full-contact practice before playing in matches.

Phase 5: Return to Full Competition (Months 6-9+)
The final phase focuses on achieving 100% return to competitive sport with ongoing injury prevention training.
Goals:
- Full return to competitive participation without modification
- Maintain strength and proprioceptive gains achieved during rehabilitation
- Implement ongoing injury prevention training
Approach:
- Full participation in team practice and competition
- Continued emphasis on warm-up protocols that emphasize ACL injury prevention
- Regular follow-up strength training (2-3 times per week) to maintain muscular balance
- Ongoing proprioceptive training incorporated into warm-ups
Return-to-Sport Criteria: We use objective criteria to clear athletes for full competition, not just time-based progression:
- Strength testing shows 95%+ limb symmetry (involved vs. uninjured leg)
- Single-leg hop testing demonstrates 90%+ limb symmetry (using single-leg hop distance)
- Y-Balance Test shows no deficits
- Sport-specific movement screening shows no compensations
- Psychological readiness questionnaire (ACL-Return to Sport after Injury Scale) shows confidence in the knee
- Clearance from both the athlete’s physician and physical therapist
ACL Recovery Without Surgery: Non-Surgical Management
Not every ACL tear requires surgical reconstruction. Some athletes, particularly those with incomplete tears or lower activity demands, can successfully rehabilitate and return to sport through conservative (non-surgical) management.
Non-surgical ACL rehabilitation emphasizes aggressive strengthening, proprioceptive training, and movement pattern correction. Success depends largely on athlete compliance with the rehabilitation program and honest assessment of their activity demands. An athlete who can commit to diligent home exercise and structured physical therapy has a better chance of successful non-surgical recovery.
However, athletes with complete ACL tears who want to return to competitive sports involving cutting, jumping, and rapid direction changes typically benefit from surgical reconstruction. The decision between surgical and non-surgical management should be made in consultation with an orthopedic surgeon and physical therapist, with consideration of the athlete’s age, competitive demands, and personal goals.
At Trinity Rehab Wayne, we provide equally comprehensive rehabilitation whether our patients choose surgical reconstruction or conservative management. The phases described above apply to both pathways, though the timeline may vary.
Essential ACL Recovery Exercises: A Sample Program
While a comprehensive rehabilitation program requires professional guidance tailored to your specific injury and timeline, here are some foundational exercises that form part of Phase 2-3 ACL rehabilitation.
Quadriceps Sets:
- Sit with your leg extended, place a small rolled towel under your knee
- Tighten your thigh muscle (quadriceps) and hold for 5 seconds
- Relax and repeat 10-15 times
- Perform 3 times daily
Glute Bridges:
- Lie on your back with knees bent and feet flat on the floor
- Push through your heels and raise your hips until your body forms a straight line from knees to shoulders
- Hold for 2 seconds at the top, lower and repeat
- 3 sets of 15 repetitions
Side-Lying Leg Lifts:
- Lie on your side with the uninjured leg bent
- Lift the injured leg (keeping it straight) 12 inches
- Hold for 2 seconds, lower and repeat
- 3 sets of 15 repetitions per side
Mini-Squats (Phase 2-3):
- Stand with feet shoulder-width apart
- Bend your knees to 30-45 degrees (quarter squat depth)
- Keep your weight in your heels and chest up
- Return to standing, repeat
- 3 sets of 12-15 repetitions
Single-Leg Balance (Phase 3+):
- Stand on your injured leg with your other knee bent
- Maintain balance for 30-60 seconds
- Progress to standing on foam or balance pad
- These exercises form a foundation, but comprehensive ACL rehabilitation involves many additional exercises tailored to your specific needs, tissue healing timeline, and sport demands.
Ice Sports and ACL Injuries: Wayne’s Hidden Risk Factor
Wayne has a unique ice sports culture. The Ice Vault arena—a figure skating training facility that has produced nationally competitive skaters and housed training by renowned athletes like Johnny Weir—represents a significant part of our community’s athletic identity. Beyond figure skating, Wayne has robust youth and adult hockey programs, recreational ice skating, and a growing population of athletes who compete across multiple ice sports.
Ice sports create ACL injury patterns and risks that are distinctly different from field or turf-based athletics, and these patterns are under-recognized in many rehabilitation settings.
Why Ice Sports Create Unique ACL Stress
The ice surface presents biomechanical demands unmatched by any other athletic environment. Unlike grass, turf, or concrete, ice provides extremely low friction. This changes how athletes can generate, absorb, and decelerate forces.
In Figure Skating: The most demanding ACL moments occur during takeoff and landing of jumps. A figure skater attempting a triple lutz generates tremendous rotational force through the body while maintaining a planted blade on ice. The landing requires deceleration of rotational momentum while supporting full body weight on a single blade. If the landing goes awry—the blade catches wrong, the leg buckles slightly, the rotational timing is off—the ACL experiences extreme varus (outward) or valgus (inward) stress. Unlike other jumping sports where athletes can adjust their body position mid-flight, figure skaters commit to their jump trajectory early, leaving little room to compensate if something goes wrong.
Additionally, the repetitive nature of figure skating training creates cumulative stress. Elite-level skaters practice jumps hundreds of times weekly. Each landing is a moment of ACL stress. The accumulated effect of thousands of jumps across a training season creates risk that extends beyond any single jump.
In Ice Hockey: Hockey creates ACL injury risks through different mechanisms. The sport demands rapid accelerations and decelerations—a player accelerates hard to chase a puck, then plants a skate blade to decelerate and change direction. The planted blade catches the ice, but the body’s momentum continues—this moment creates massive shear force across the knee. Additionally, hockey involves body checking and contact. While a direct collision might cause an injury, more commonly the lateral forces of being checked—or of checking an opponent—drive the knee into an unstable position.
Hockey’s demands also include “edge work”—the ability to carve and maneuver on the edges of the skate blade rather than flat. This edge work, while providing superior skating performance, requires greater hip and ankle stability to prevent the blade from slipping and the knee from compensating with valgus collapse.
ACL Injury Risk Factors Specific to Ice Sports
Athletes in ice sports face particular risk factors:
Blade Design and Fit: The blade is the only contact point between the athlete and the ice. If the blade is dull, misaligned, or poorly fitted, the athlete must over-compensate with hip and knee musculature. Younger athletes, particularly in Wayne PAL-affiliated programs, sometimes use equipment that doesn’t fit optimally—hand-me-down skates, poorly maintained blades, or sizing that prioritizes cost over performance. This creates ACL injury risk.
Training Volume: Figure skaters pursuing competitive skating train 15-25+ hours weekly on ice. Hockey players compete in multiple leagues (school team, club team, recreational league) plus private coaching. This volume of ice-specific movement creates cumulative ACL stress.
Movement Retraining Challenges: Unlike field athletes who can modify movement patterns immediately, ice athletes must adapt their entire kinetic chain to the constraints of ice. A hockey player cannot suddenly “play more careful”—the skating demands remain unchanged. This makes injury prevention more challenging.
Blade Catches and Unexpected Events: Figure skaters occasionally experience moments where the blade catches the ice unexpectedly, particularly during transitions between different moves or when executing moves near the boards or on different ice surfaces. These unexpected catches can produce rapid, extreme forces that tear the ACL.
ACL Rehabilitation for Ice Sports Athletes
Rehabilitating ice sports athletes requires specific considerations. The return-to-ice timeline differs from return-to-field sports because skating places unique demands on knee stability that land-based sports don’t.
Specifically, ice athletes must progress through a landing/takeoff rehabilitation phase before returning to ice. For figure skaters, this means controlled, progressive jump training on land before returning to ice jumps. For hockey players, this means progression from stationary skating to accelerating, to lateral movements, to sport-specific drills.
At Trinity Rehab Wayne, we have specific experience rehabilitating ice sports athletes because of our community’s Ice Vault culture. We understand that a hockey player cleared for “running and cutting” drills isn’t automatically ready to return to ice—the skating demands require additional progression. Similarly, a figure skater cleared for jumping mechanics drills needs ice-specific proprioceptive training and carefully structured jump progression on ice before returning to competitive jump training.
We coordinate closely with skate coaches and hockey coaches to ensure that return-to-ice progression is structured appropriately. We’ve developed specific protocols for:
- Stationary skating balance and stability
- Forward and backward skating with progressive speed
- Lateral skating and crossovers
- Stopping and starting movements (particularly critical for hockey)
- Jump progression for figure skaters (single jumps before double or triple attempts)
- The decision about when to progress through these ice-specific phases is guided by objective criteria—strength testing, hop testing, proprioceptive assessment—not just pain-free tolerance or subjective readiness.
Why Choose Trinity Rehab Wayne for Your ACL Recovery
Trinity Rehab’s Wayne location on Hamburg Turnpike serves our community’s athletes with specialized expertise in ACL rehabilitation and return to sport. Here’s what sets our approach apart:
- Sport-Specific Experience: Our physical therapists have extensive experience rehabilitating Wayne’s unique athletic population—athletes navigating the two-school rivalry, ice sports enthusiasts training at Ice Vault, and young athletes coming through Wayne PAL programs. We understand the specific demands athletes in our community face.
- Comprehensive Assessment: Every ACL rehabilitation program at Trinity Rehab Wayne begins with comprehensive movement screening and assessment. We identify not just the ACL injury itself, but the underlying movement deficits, muscle imbalances, and compensations that may have contributed to the injury. This comprehensive assessment ensures our rehabilitation addresses root causes, not just symptoms.
- Evidence-Based Protocols: Our ACL rehabilitation follows the latest evidence and research. We don’t rely on outdated time-based progression; instead, we use objective testing—strength testing, hop testing, movement quality assessment—to determine progression.
- Progressive Return-to-Sport: We work closely with athletes, parents, and coaches to develop realistic, progressive return-to-sport plans. We won’t clear an athlete for full competition before they meet objective criteria, even if they’re eager to return. We also won’t delay return unnecessarily—our goal is safe, timely return to the sport you love.
- Psychological Support: ACL injuries carry psychological weight, particularly for competitive young athletes in a high-pressure environment like Wayne. Our therapists address the psychological dimensions of recovery, helping athletes rebuild confidence in the knee.
- Coordination with Medical Providers: Whether your athlete chose surgical reconstruction or conservative management, we coordinate closely with their orthopedic surgeon or physician. Regular communication ensures rehabilitation is progressing appropriately and aligned with medical recommendations.
- Convenient Location: Our Hamburg Turnpike location is accessible to athletes across Wayne and surrounding communities in Passaic County. We offer flexible scheduling to accommodate school and practice commitments.
The Role of Mental Health and Psychology in ACL Recovery
Physical rehabilitation following an ACL injury addresses the structural, muscular, and functional aspects of recovery. However, research increasingly recognizes that psychological readiness is equally important for successful return to sport. This is particularly true for young athletes in Wayne’s competitive environment, where psychological pressure to return quickly can outpace physical readiness.
ACL injuries often trigger anxiety, fear of re-injury, and loss of confidence. An athlete who played with instinctive confidence before their injury may find themselves hesitant during cutting movements, jumping, or competitive situations weeks into their rehabilitation—not because they’re physically unprepared, but because their brain hasn’t rebuilt trust in the knee.
Inside Our Wayne Clinic




Wayne ACL Rehab For Sport, Work, And Confident Cutting
ACL rehab in Wayne often means helping athletes and active adults rebuild confidence for sprinting, jumping, pivoting, gym training, and weekend sports while also handling school, work, and family schedules.
Depending on your stage of recovery, your therapist may assess swelling, knee range of motion, quad strength, single-leg control, balance, gait, jumping and landing mechanics, cutting readiness, and surgeon precautions when post-surgical rehab is involved.
For connected knee and sport goals, see sports injury rehab in Wayne, Wayne meniscus tear treatment, and Wayne knee pain physical therapy.
Frequently Asked Questions About ACL Injury and Recovery
Do I definitely need surgery if I tear my ACL?
How long until I can return to sports?
What’s the difference between ACL and MCL injuries?
Can I do physical therapy if I don’t have surgery?
What should I do immediately after tearing my ACL?
Can I re-tear my ACL after recovery?
How much does ACL rehabilitation cost?
What if I’m not an athlete—will I still need intensive rehabilitation?
Can I do my home exercises instead of coming for therapy?
How do I know when I’m ready to return to sports?
Next Steps: Starting Your ACL Recovery Today
If you’re dealing with an ACL injury—whether diagnosed yesterday or nagging you for months—the time to act is now. Recovery is possible. Athletes return to sport. Non-athletes return to hiking, dancing, and playing with grandchildren. But recovery requires commitment, expertise, and the right support.
Here’s what we recommend:
Trinity Rehab Brick is ready to guide you through every phase of ACL recovery.
- Get a diagnosis if you haven’t already. An MRI confirms ACL injury and identifies any additional damage. See your primary care physician or an orthopedist within 48 hours of injury.
- Schedule a consultation at Trinity Rehab Woodbridge. Call us or visit our Crosspoint Town Square location at 33 Woodbridge Center Drive. We’ll discuss your goals, your sport, your lifestyle, and what recovery looks like for you specifically. We’ll answer questions and develop a plan.
- Commit to rehabilitation. Whether surgery or conservative treatment, recovery requires effort. Plan for 2-3 sessions weekly for several months. Plan for home exercises most days. This is your investment in returning to the activities you love.
- Trust the process. Rehabilitation has a proven timeline for a reason. Pushing too hard too fast risks re-injury. Following the plan, doing the work, and progressively challenging yourself—this approach works.
You live in Woodbridge, a diverse, athletic community with world-class fitness facilities and incredible talent. Whether you’re a Barron or a recreational player, a high school student or a 55-year-old weekend warrior, you deserve professional ACL care from people who understand your sport, your community, and your goals.
Trinity Rehab Woodbridge is here to get you back. Let’s start today.